A study published on December 23, 2025, in Neurology, the medical journal of the American Academy of Neurology, examined how age may influence recovery following a spinal cord injury.
“With population growth and improvements in medicine, the…
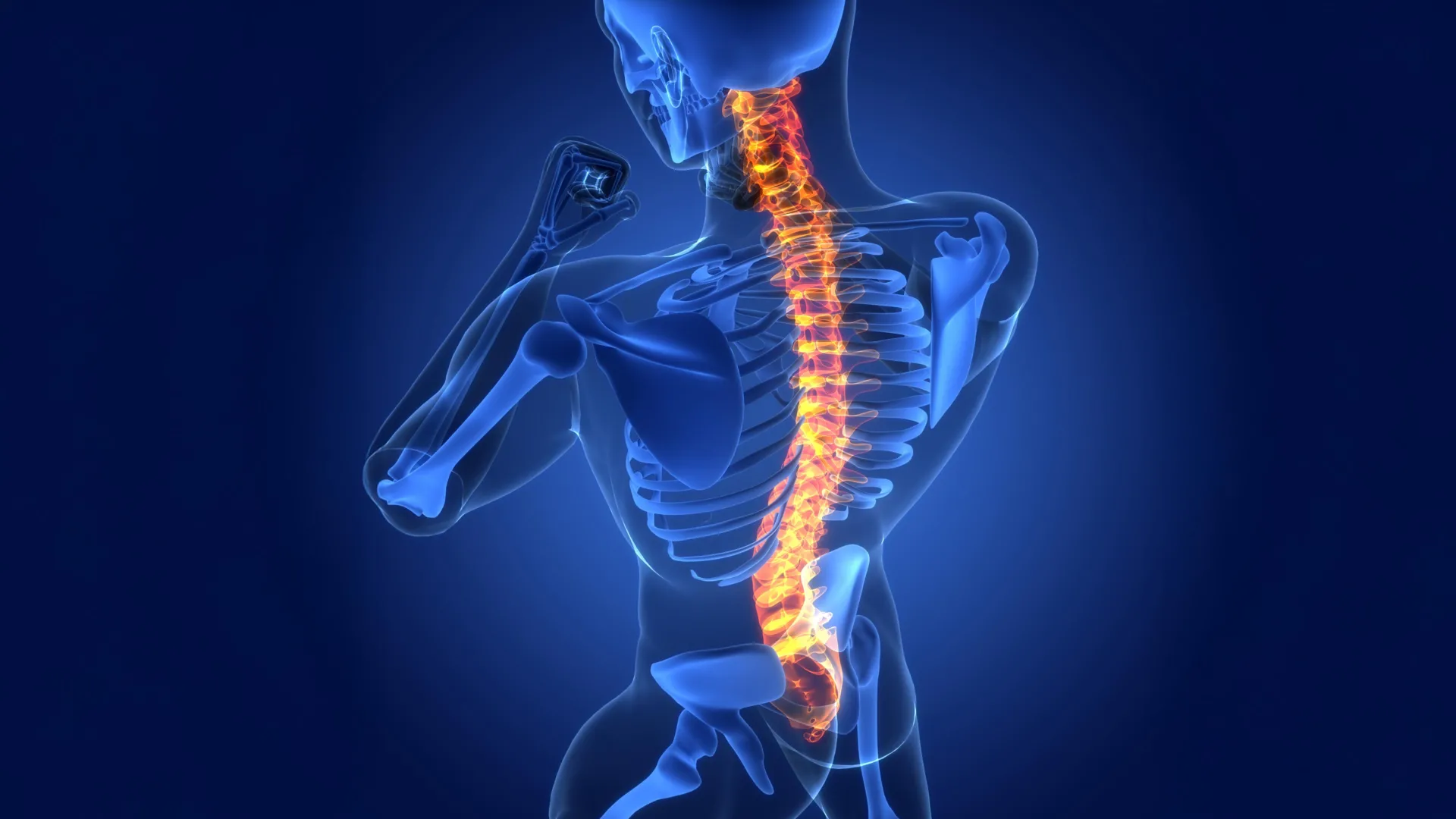
A study published on December 23, 2025, in Neurology, the medical journal of the American Academy of Neurology, examined how age may influence recovery following a spinal cord injury.
“With population growth and improvements in medicine, the…
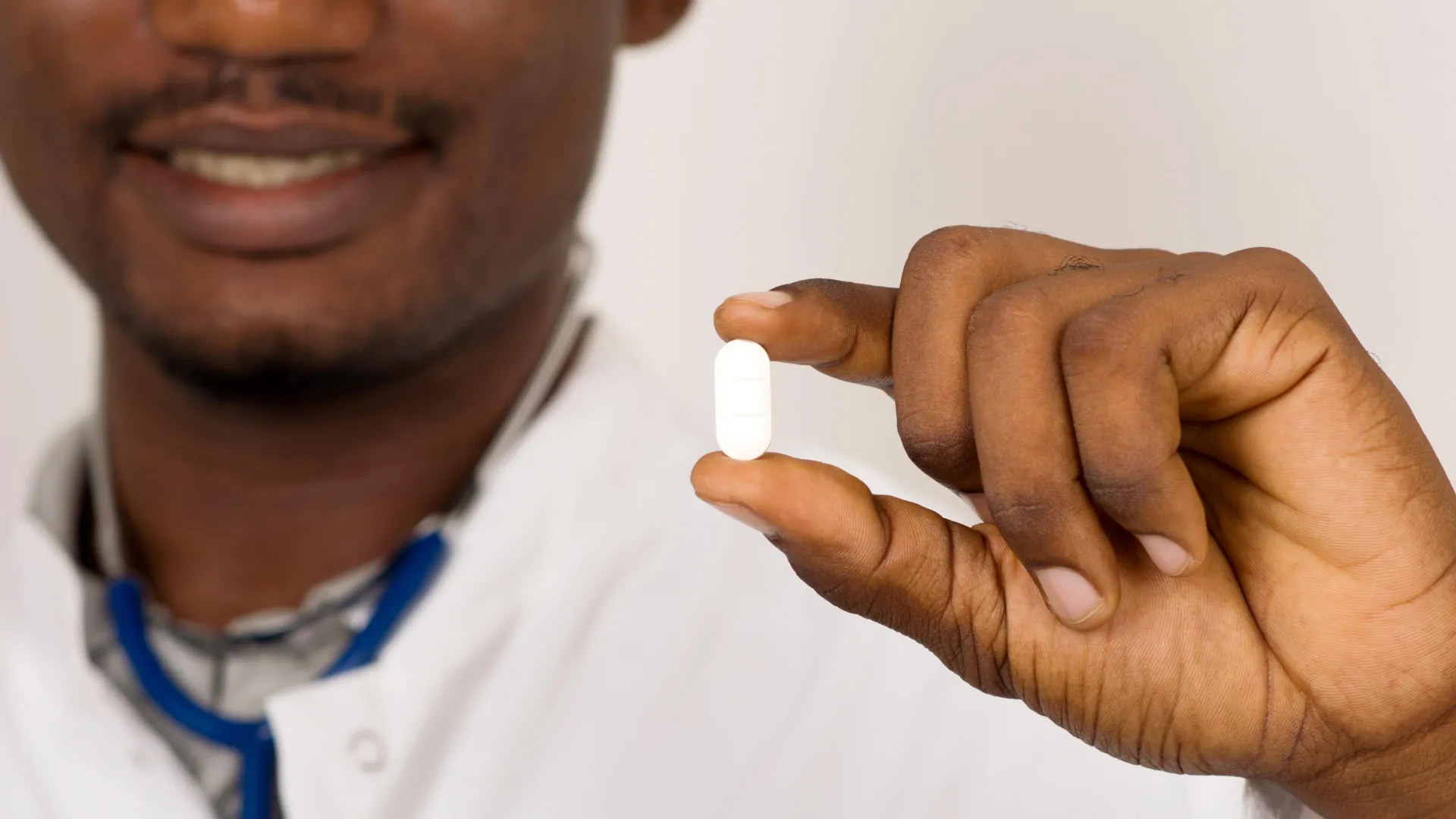
Researchers are testing a new oral medication called zoliflodacin that could offer a simpler way to treat gonorrhea, especially strains that no longer respond well to existing antibiotics. In a late-stage phase 3 clinical trial published in The…
Nickbakhsh, S. et al. Epidemiology of seasonal coronaviruses: establishing the context for the emergence of coronavirus disease 2019. J. Infect. Dis. 222, 17–25 (2020).
Graham, N. M. The…
Levine, A. J. p53: 800 million years of evolution and 40 years of discovery. Nat. Rev. Cancer 20, 471–480 (2020).
Kastenhuber, E. R. & Lowe, S. W. Putting p53 in context. Cell 170,…

Researchers at two West Yorkshire universities are leading a study examining ways to slow the progression of short-sightedness.
Staff at the University of Bradford and the University of Huddersfield are investigating how contact lenses worn by…

When Rob Hobson, a registered nutritionist based in the UK, found out his cholesterol levels were “really high” in June, he decided to manage them through diet, focusing particularly on increasing his fiber…
Published on
A new artificial intelligence tool could speed up the search for treatments for heart disease, according…

Scientists from Nanyang Technological University, Singapore (NTU Singapore) have found that the brain’s waste removal system often becomes blocked in people who show early signs of Alzheimer’s disease. These blockages interfere with the brain’s…
Kassebaum, N. J. et al. Global burden of untreated caries: a systematic review and metaregression. J. Dent. Res. 94(5), 650–658 (2015).
Sachdeva, A. The public health burden of untreated…