- 4 Habits You Need to Break to Help Slow Aging, According to Doctors EatingWell
- Things we should all be doing to boost health and live longer EDP24
- NIH scientist’s guide to a longer, healthier life news.cgtn.com
- Orthopaedic surgeon says ‘one per…
Category: 6. Health
-
4 Habits You Need to Break to Help Slow Aging, According to Doctors – EatingWell
-
This “Forgotten” Organ May Hold the Key to Cancer Survival – SciTechDaily
- This “Forgotten” Organ May Hold the Key to Cancer Survival SciTechDaily
- Thymic health consequences in adults Nature
- This overlooked organ may be more vital for longevity than scientists realized Scientific American
- Professor Nicolai Juul…
Continue Reading
-

Man Recalls ‘Emotional Toll’ of Having Psoriasis as a Teen: ‘It Was Very Difficult to Live and Be Out in the World’ (Exclusive)
NEED TO KNOW
-
A man recalls the emotional toll growing up with plaque psoriasis had on him as a teenager in an exclusive interview with PEOPLE
-
“It was very difficult to walk around and have these large, scaly, red masses on my body and my face,”…
Continue Reading
-
-
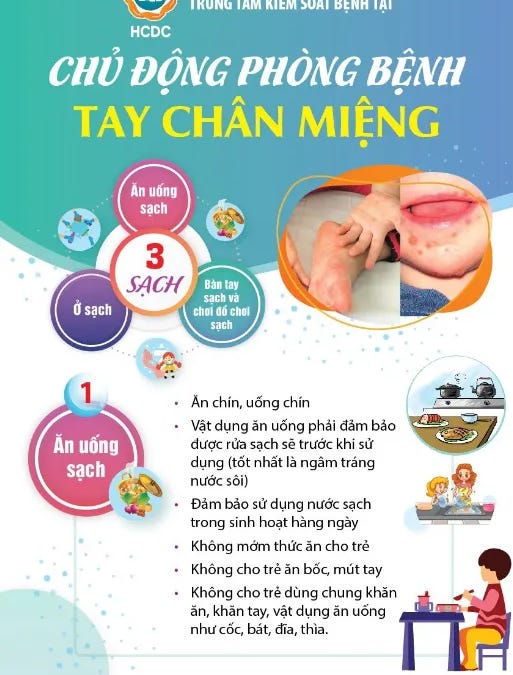
Sharp increase in hand, foot, and mouth disease hospitalizations
Recently, hand, foot, and mouth disease (HFMD) has been rapidly increasing. According to records from the National Children’s Hospital in Hanoi, in just the first two months of 2026, nearly 3,000 children contracted the disease, with about…
Continue Reading
-

Panama calls on public in battle with dengue
The Panama Ministry of Health (MOH) is calling on the public to reinforce prevention measures and eliminate breeding grounds for the mosquito that transmits dengue fever.
Image/CDC According to the Department of Epidemiology of the MOH, in the…
Continue Reading
-

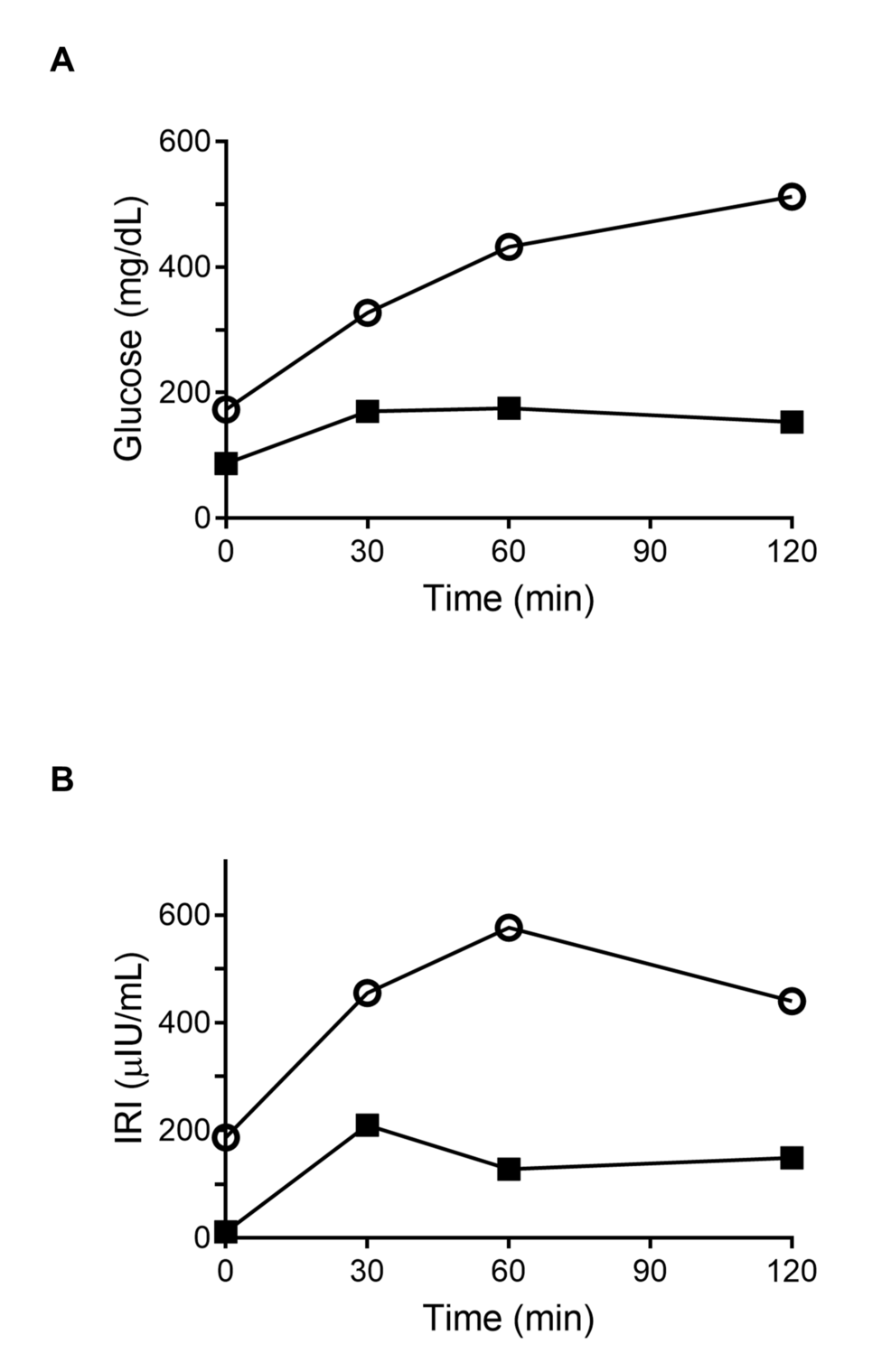
Keto restores oxygen use and muscle response to exercise
A new study has found that a ketogenic diet can restore a major training benefit that high blood sugar had shut down in mice, allowing exercise to raise oxygen use again.
That finding recasts the problem of exercise resistance, suggesting that…
Continue Reading
-

“Silent mode” phone users share similar psychological traits
A new study from Kyung Hee University explores how phones in “silent mode” may hold the key to healthier minds at work.
Researchers examined whether a mobile mindfulness training (MMT) program could improve stress, burnout, and work…
Continue Reading
-
Eating less protein may slow tumor growth in damaged livers
Researchers have found that cutting dietary protein slows liver tumor growth in mice whose damaged livers cannot clear ammonia properly.
The finding recasts a routine part of eating as a source of fuel for cancer when the organ meant to neutralize…
Continue Reading
-

Pre-workout supplements linked to extreme sleep loss
A new study has found that young people who use pre-workout supplements are more than twice as likely to sleep five hours or less a night.
That finding recasts a familiar gym aid as a possible driver of severe sleep loss during years when rest…
Continue Reading