- Video: AI advances help care teams find hard-to-see colon polyps Medical Xpress
- Preventing Colon Cancer | VA Minneapolis Health Care | Veterans Affairs VA.gov Home | Veterans Affairs
- Improving access to team-based health care for Tri-Cities…
Category: 6. Health
-
Video: AI advances help care teams find hard-to-see colon polyps – Medical Xpress
-
Gut Bacteria May Directly Enter The Brain, Study in Mice Reveals : ScienceAlert
Past studies have found that gut activity can have significant impacts on the brain, and vice versa.
Now, new research in mice explains how some of that communication might occur: through very small numbers of live bacteria traveling from the…
Continue Reading
-
Discovery might inform new approach to Huntington's disease – Medical Xpress
- Discovery might inform new approach to Huntington’s disease Medical Xpress
- Findings may inform new approach to Huntington’s disease UW Medicine | Newsroom
- Huntington’s Disease May Be Driven by Toxic HTT1a Protein Fragment Inside Precision…
Continue Reading
-

Brain scans reveal diet linked to slower brain aging
Aging does not happen all at once. Some days feel the same, but inside the brain, changes keep building over time. These shifts are slow and easy to miss.
Brain tissue gradually shrinks. Spaces inside the brain grow larger. Parts that once worked…
Continue Reading
-
Menopause Before Age 40 Linked to Higher Risk
Share on Pinterest Premature menopause has been linked to a higher risk of coronary artery disease. FG Trade/Getty Images - Women who go through natural menopause before age 40 face a 40% higher lifetime risk of coronary heart disease.
- Black women are…
Continue Reading
-
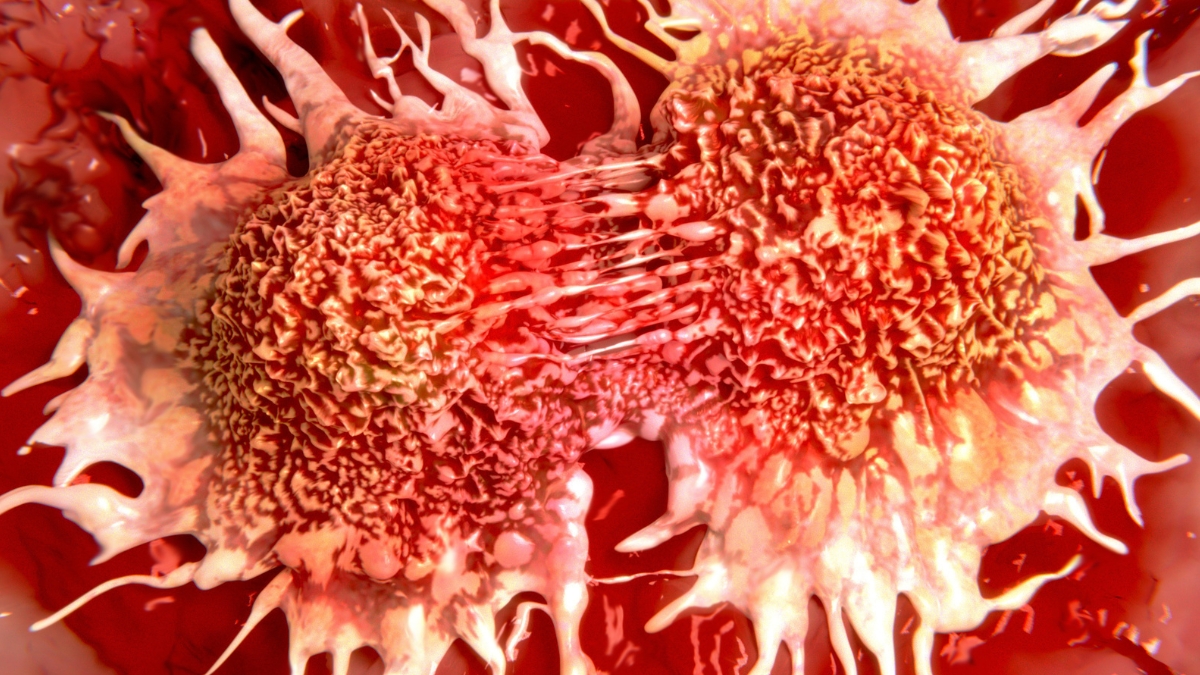
New Experimental Drug Shrinks Tumors in Prostate Cancer Clinical Trial : ScienceAlert
A new immunotherapy drug has demonstrated early promise in a recent prostate cancer clinical trial. The drug, called VIR-5500, is a “masked T-cell engager”. This type of immunotherapy ignites our own immune arsenal to fight cancer.
In the…
Continue Reading
-

RARC Surgical Smoke Shows No Cancer Spread Risk
CONCERNS about the potential spread of cancer during minimally invasive surgery may be unfounded, according to new research investigating surgical smoke generated during robot-assisted radical cystectomy (RARC) for bladder cancer.
RARC is…
Continue Reading
-

NCCS is Making Waves in Colorectal Cancer Research- National Cancer Centre Singapore
National Cancer Centre Singapore shared a post on LinkedIn:
“NCCS is making waves in colorectal cancer research!
Colo-SCRIPT (Colorectal cancer subtype-specific research informs phenotypes, diagnostics & treatments) secured a…
Continue Reading
-

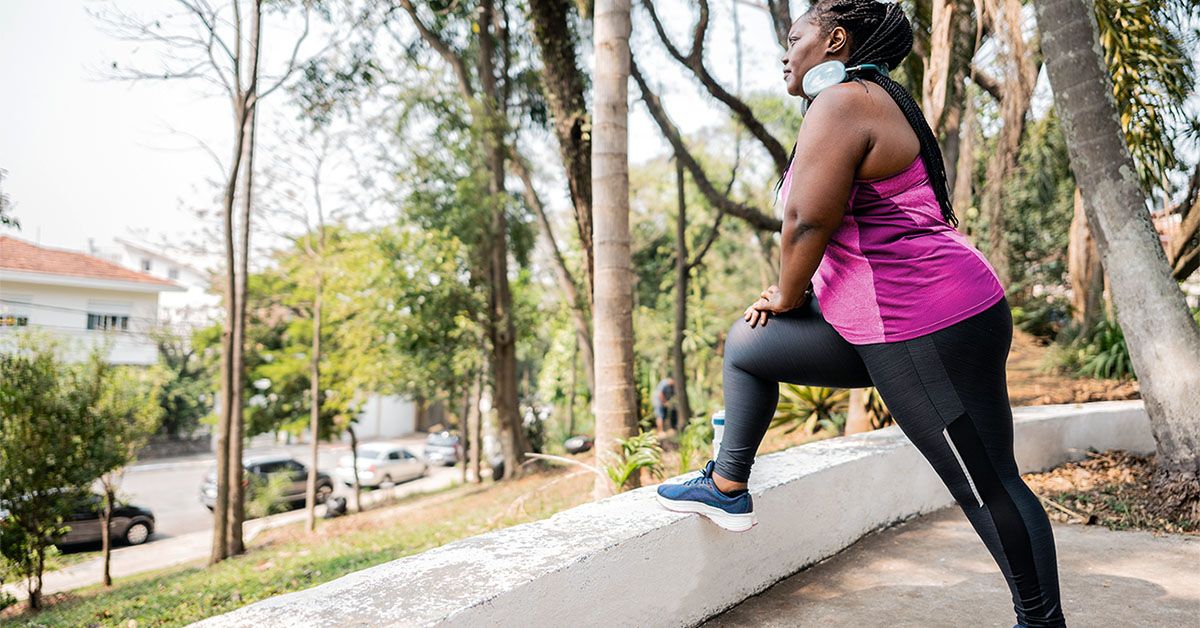
Weekly HIIT Exercise Could Improve Memory, Study Finds
25
Exercise is widely considered one of the most effective ways to maintain a healthy, fit, and active body. It not only helps improve strength, stamina, and flexibility but also plays a key role in preventing various…
Continue Reading
-

Brown algae extracts show strong antioxidant potential
Photo: Nuqo A dual in vitro and in vivo study reveals promising effects of Ascophyllum nodosum and Fucus vesiculosus on oxidative stress modulation.
As livestock production systems evolve under the dual pressures of sustainability and performance,…
Continue Reading