The beginning of every new year comes with resolutions and a vow…
Category: 6. Health
-
Experts warn U.S. risks losing measles elimination status
(Xinhua) 15:04, December 31, 2025NEW YORK, Dec. 31 (Xinhua) — A measles outbreak was reported in the U.S. state of South Carolina on Tuesday, and health experts warned that the country risks losing its elimination status if the…
Continue Reading
-

Find out how you’re harming your kid with screen time
Screen time is affecting your toddler more than you know.
Children exposed to high levels of…
Continue Reading
-

Leicestershire farmer one of UK’s first in trial to treat aneurysms
 University of Leicester
University of LeicesterPhilip Gosling said when researchers told him about the trial “I had to get involved” A farmer is among the first people in the UK to join a trial which is testing whether a diabetes drug can treat a “deadly” form of…
Continue Reading
-

Leicestershire farmer one of UK’s first in trial to treat aneurysms
Mr Gosling, from Leicestershire, joined the trial in July after being referred to Prof Matt Brown, who is leading the UK’s branch of the trial.
He was told his AAA, a balloon-like swelling in the abdominal portion of the body’s main artery, was…
Continue Reading
-

‘My hoarding is not a lifestyle choice, it’s a mental health issue’
Bea SwallowWest of England
 Handout
HandoutHoarding was recognised as a complex mental health condition in 2013 A sliver of space left on a mattress, narrow winding pathways carved through clutter and precarious piles of newspapers – this is just a small…
Continue Reading
-
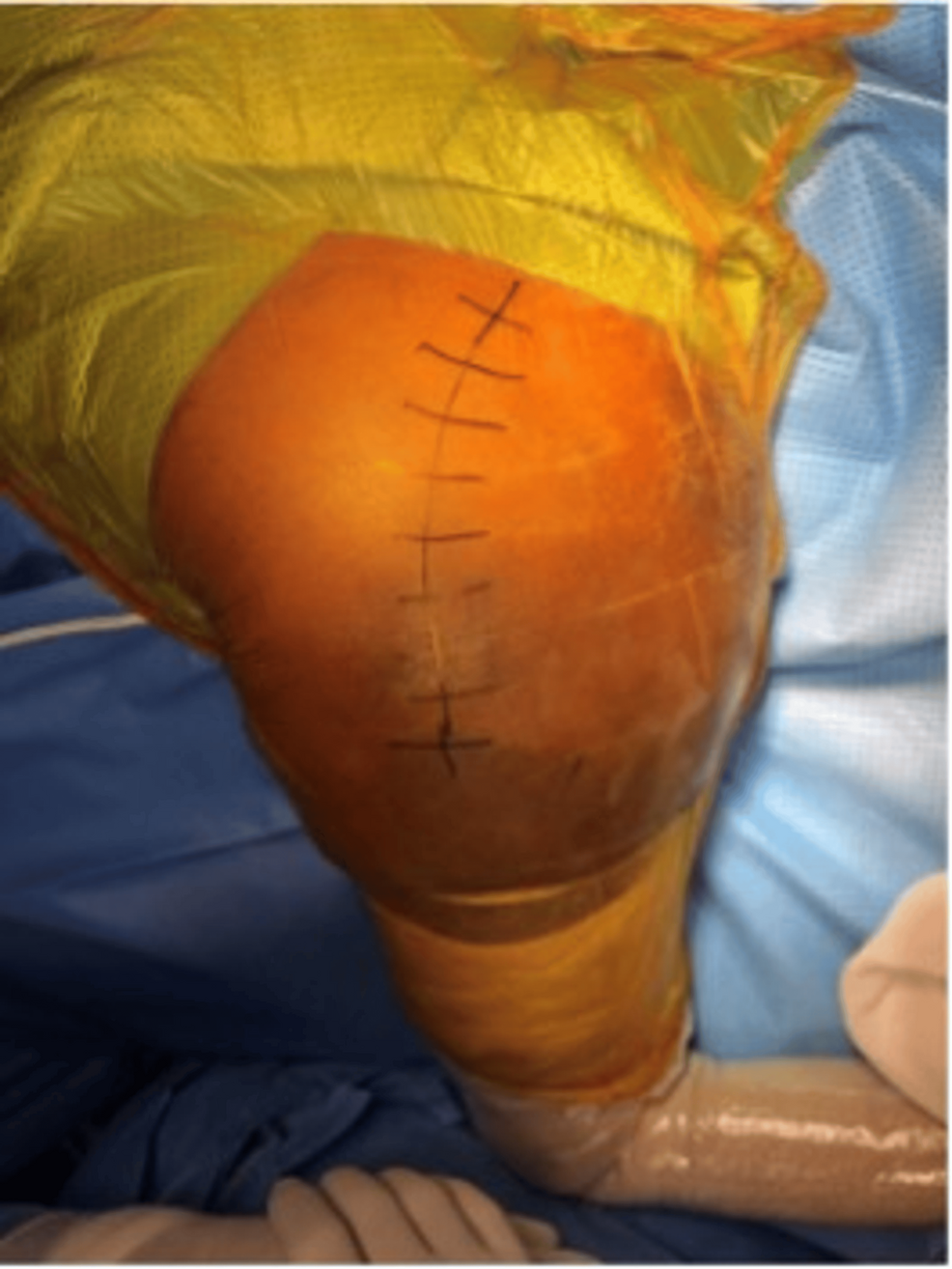
Welder’s Anthrax Treated with Obiltoxaximab — Louisiana, 2024
Investigation and Findings
Identification of Patient
On September 7, 2024, CDC and the Louisiana Department of Health (LDH) were contacted by a clinician regarding an otherwise healthy man aged 18 years from Louisiana, who was being admitted to…
Continue Reading
-

Parkinson’s diagnosis ‘hangs like a cloud’, says Suffolk teacher
 Supplied
SuppliedSchool teacher Sam Sharp said being diagnosed with Parkinson’s came as a “huge shock” Sam Sharp was once a keen runner and walker who had conquered testing terrains and scaled mountains across the world.
But, in February 2024, the Suffolk…
Continue Reading
-
Immuno-acoustic trapping for extracellular vesicle subpopulations
Charrin, S., Jouannet, S., Boucheix, C. & Rubinstein, E. Tetraspanins at a glance. J. Cell Sci. 127 (17), 3641–3648 (2014).
Fan, Y. et al. Differential proteomics argues against a general…
Continue Reading