Zhang, H. Y., Bi, W. G., Yu, Y. & Liao, W. B. Angelica sinensis (Oliv.) Diels in China: Distribution, cultivation, utilization and variation. Genetic Res. Crop Evol. 59(4), 607–613. https://doi.org/10.1007/s10722-012-9795-9 (2012).
Category: 6. Health
-

Super influenza: Symptoms, treatment, and prevention
As flu cases surge worldwide, health experts are warning about super influenza, a more aggressive form of the flu that spreads rapidly and causes severe complications.
Doctors say early recognition and proper care…
Continue Reading
-

Effects of Remimazolam on Perioperative Inflammatory Response and Neur
Introduction
Perioperative Neurocognitive Disorders (PND), particularly postoperative delirium, delayed neurocognitive recovery, and postoperative neurocognitive disorders, not only hinder recovery and significantly impair patients’ self-care…
Continue Reading
-

Film raises empathy and awareness for youths with virus
Students hold a red ribbon, the symbol of AIDS support, during an event to raise awareness about the virus at the University of South China in Hengyang, Hunan province, in November.[Photo provided by Cao… Continue Reading
-

The brain has a hidden language and scientists just found it
Scientists have developed a protein that can record the chemical messages brain cells receive, rather than focusing only on the signals they send out. These incoming signals are created when neurons release glutamate, a neurotransmitter that…
Continue Reading
-
The brain has a hidden language and scientists just found it
Scientists have developed a protein that can record the chemical messages brain cells receive, rather than focusing only on the signals they send out. These incoming signals are created when neurons release glutamate, a neurotransmitter that…
Continue Reading
-
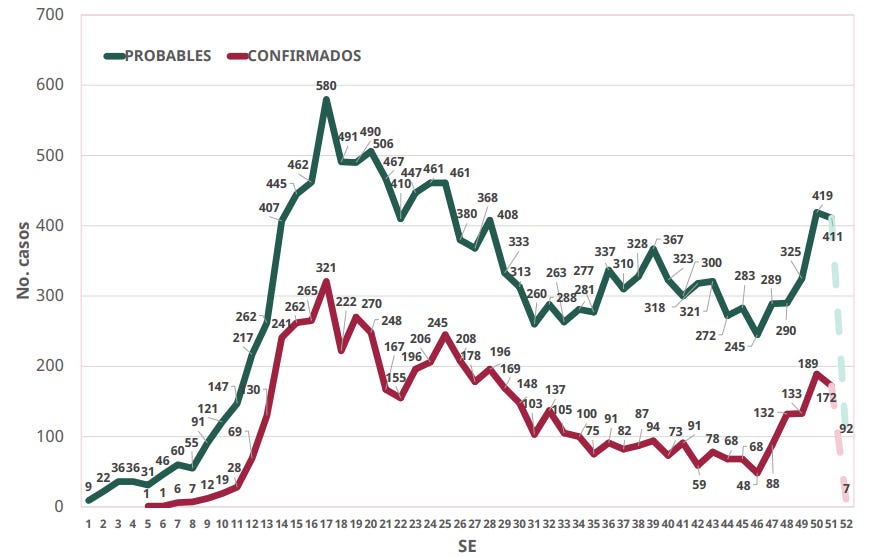
Mexico confirmed measles total tops 6,000 cases in 2025
According to the Mexico Ministry of Health, 6,050 cumulative confirmed cases of measles from 29 states and 207 municipalities through December 26 this year.
Of the confirmed cases*, states reporting the most include Chihuahua (4,481), Jalisco…
Continue Reading
-

Journal of Medical Internet Research
Introduction
There is limited research examining the sexual and reproductive health (SRH) experiences of cisgender, lesbian, bisexual, and queer (LBQ+) women of color in the United States. Historically, research about the SRH experiences of sexual…
Continue Reading
-
U.S. Surpasses 2,000 Measles Cases This Year—Most Since 1992 – Forbes
- U.S. Surpasses 2,000 Measles Cases This Year—Most Since 1992 Forbes
- Newark Airport passenger may have exposed others to measles, New Jersey Health Department says ABC7 New York
- Holiday travelers at US airport ‘exposed to world’s most infectious…
Continue Reading
