Introduction
The role of obesity for health is an important matter because the prevalence of adult obesity in 2022 has doubled since 1990 and that of adolescents quadrupled.1 Numerous studies assessed the relation of weight and disease-free…
The role of obesity for health is an important matter because the prevalence of adult obesity in 2022 has doubled since 1990 and that of adolescents quadrupled.1 Numerous studies assessed the relation of weight and disease-free…
Herpes zoster (HZ) is a skin disease caused by the infection of the spinal cord and cranial nerves by the varicella-zoster virus (VZV). It is characterized by vesicular eruptions along the affected dermatomes, accompanied by…
Every week, the NeurologyLive® staff prepares this preview of what to expect from our coverage. This week on NeurologyLive, there are a number of hot topics that we will be posting on the website. As always, our weekly coverage extends beyond…
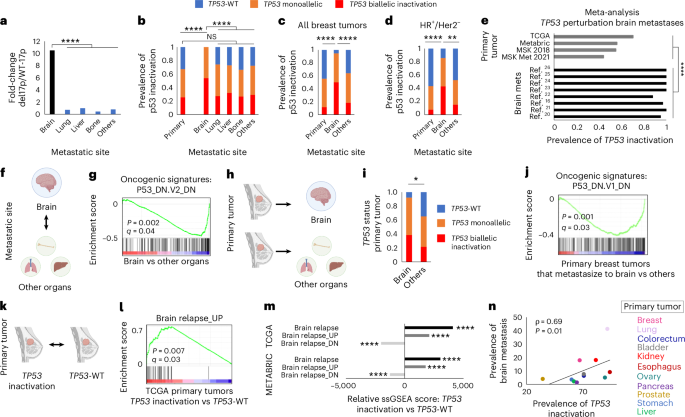
Harbeck, N. et al. Breast cancer. Nat. Rev. Dis. Primers 5, 66 (2019).
Google Scholar
Chen, W., Hoffmann, A. D., Liu, H. & Liu, X. Organotropism: new insights into molecular…

Depression is often linked to grief, financial stress, or unemployment. But for many people, the sadness arrives without a clear reason. Research suggests that several everyday factors—often ignored—may quietly…

There is “no evidence” drugs used to treat menopausal women either increases and slashes the risk of dementia, researchers have said.
A study conducted by University College London, with support from the University of Exeter, reviewed whether…

A recent study underscores the significant link between sleep apnoea and an increased risk of mental health conditions in older adults. The research, conducted on over 30,000 Canadians aged 45-85, shows a striking 40% higher probability of…