Research Highlights:
- A study of nearly 300 thousand adults in South Korea found that individuals with higher blood pressure (≥120 mm Hg/80 mm Hg) for up to 10 years during young adulthood (ages 30 and 40 were more likely to…

Research Highlights:
Applying artificial intelligence techniques to cardiac ultrasound data may make it easier to identify patients with advanced heart failure, a new study has found. The study—led by investigators at Weill Cornell Medicine, Cornell…

A NEW clinical study suggested that faecal microbiota transplantation (FMT) enhanced treatment response in adults experiencing depressive episodes when used alongside standard medication.
Depression remains a leading contributor to global…
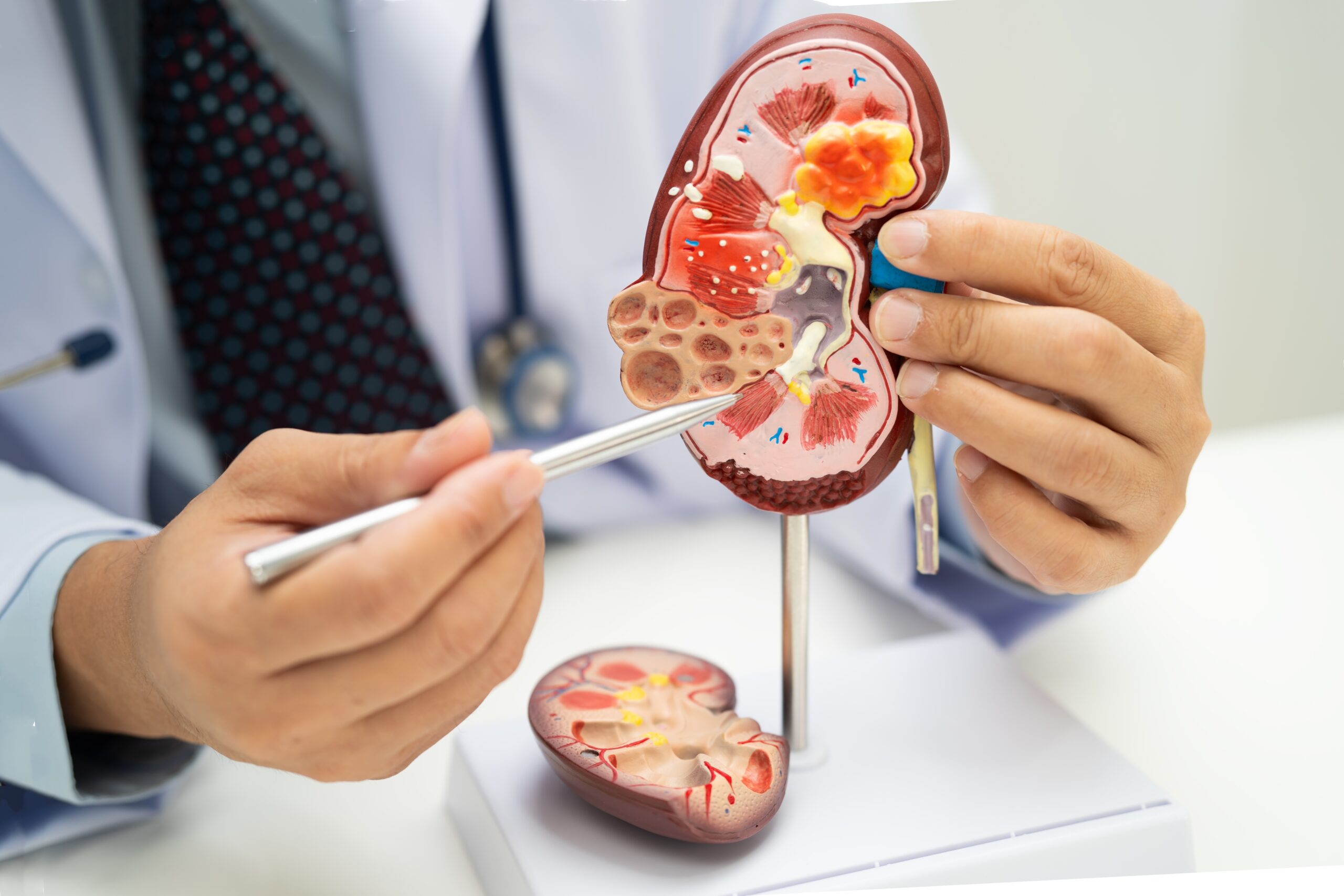
Scientists have discovered how an imbalance in gut bacteria can accelerate chronic kidney disease, with early findings pointing to a potential drug that could interrupt the damaging cycle and improve outcomes.

Researchers have…

The FIBROSIS-4 (FIB-4) index may not reliably identify liver fibrosis in people with metabolic dysfunction-associated steatotic liver disease (MASLD), according to a primary care study in Belgium and the Netherlands.
MASLD, previously known as…
(Yicai) March 20 — Chinese researchers have developed a mitochondrial capsule that can safely and efficiently deliver the tiny energy-producing organelles into cells and tissues, opening a new therapeutic avenue for diseases, including…

Can babies grow normally without eating animal foods? For many families choosing vegan or vegetarian diets, that question has remained a constant concern during the earliest and most vulnerable years of life.
A new analysis of nearly 1.2 million…
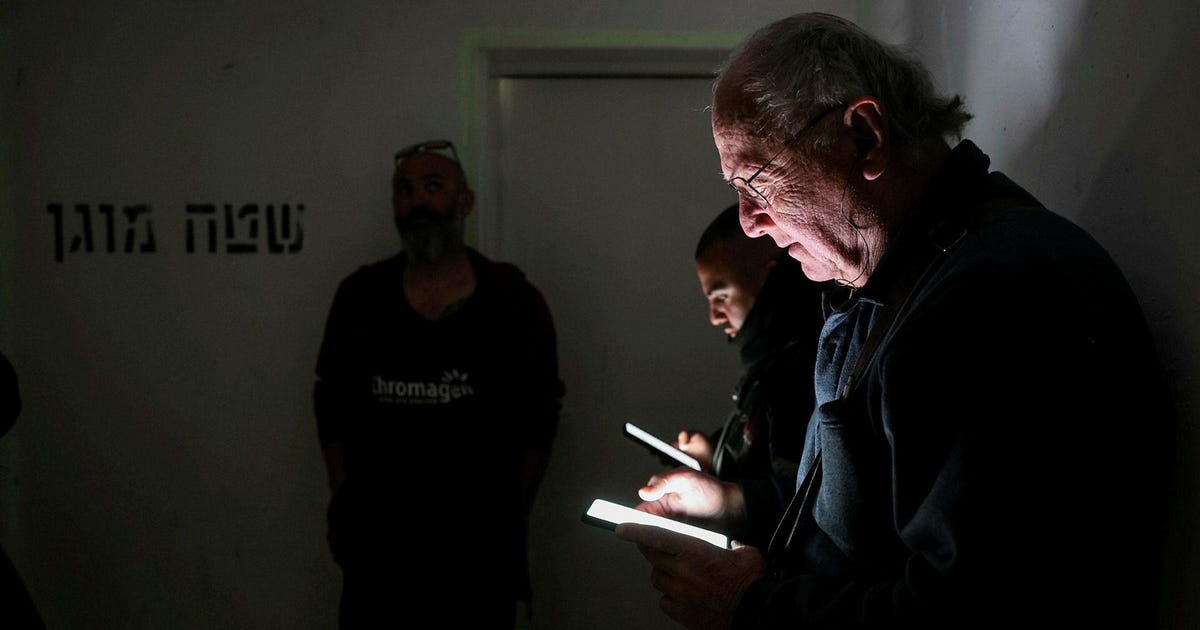
By now, this has become a daily challenge: how many hours of sleep can one get in a night riddled with air-raid alerts, racing to shelter and attempts at shuteye before being woken up again. And not just how many hours in total, but also how long…

Sleep tracking apps can cause stress for people with insomnia as they heighten awareness of sleep quality and monitoring, according to a new study.
ADVERTISEMENT