Category: 6. Health
-

Measles outbreak kills three children in Dherki
At least three children have died in a deadly measles outbreak in the village of Jan Mohammad Mehar in Dherki, while 10 others have been hospitalised, reported 24NewsHD TV Channel on Sunday.
The deceased children were identified as Amir Ali,…
Continue Reading
-

Steroid use is ‘exploding’ in Australia – but there are no clinical guidelines on how to quit
By Charmayne Allison, ABC News
Long-term steroid use can lead to cardiovascular issues, poor liver function, kidney failure and mental illness.
Photo: ABC News: Mark LeonardiWorking to calm his breathing, George Napper bent down to…
Continue Reading
-

DNA Methylation Patterns Linked to Gestational Diabetes Identified Across Pregnancy Stages – geneonline.com
- DNA Methylation Patterns Linked to Gestational Diabetes Identified Across Pregnancy Stages geneonline.com
- New Clues Reveal How Gestational Diabetes Affects Offspring Eurasia Review
- Early Screening For Gestational Diabetes: Why Timely Detection…
Continue Reading
-

The Best Evening Habit to Support Digestion
- Unwind in the evening with a warm cup of herbal tea to support healthy digestion.
- Herbal teas like peppermint, ginger and fennel may ease discomfort and constipation risk.
- Eating fiber-rich foods, managing stress and staying active are also…
Continue Reading
-
Newark Airport passenger may have exposed others to measles, New Jersey Health Department says
NEWARK, New Jersey (WABC) — A passenger at Newark Airport may have exposed people to measles.
New Jersey’s Health Department says someone with the disease passed through the airport on Friday, December 19.
The person was in terminals B and C…
Continue Reading
-
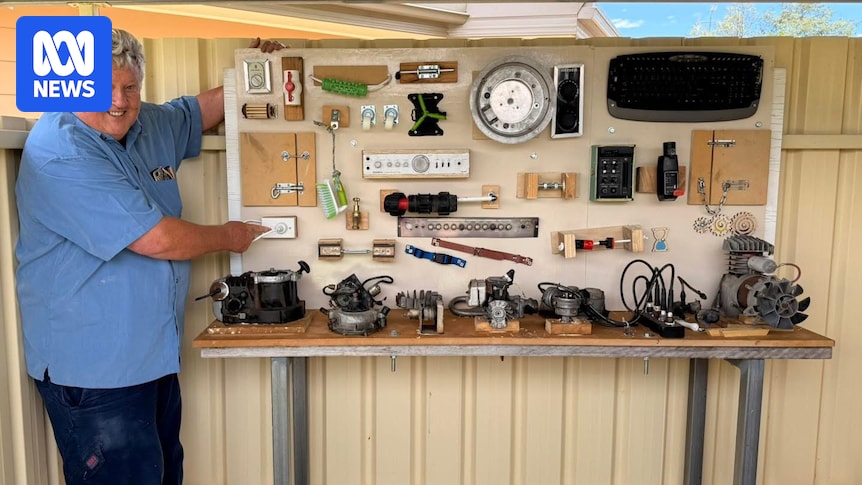
Hands-on memories spark connection for dementia residents at western NSW aged care home
Creating meaningful, sensory activities for people living with dementia can be challenging, particularly when many traditional options feel more suited to children than adults with a lifetime of lived experience behind them.
At Cooinda Aged Care…
Continue Reading