The researchers in a recent breakthrough have discovered a…
Category: 6. Health
-

Which Is Better for Your Blood Sugar?
- Scrambled eggs are high in protein and will have little impact on blood sugar response.
- Oatmeal contains fiber and your blood sugar response may depend on the type of oats you choose.
- Both are healthy breakfast options; pairings and mix-ins…
Continue Reading
-

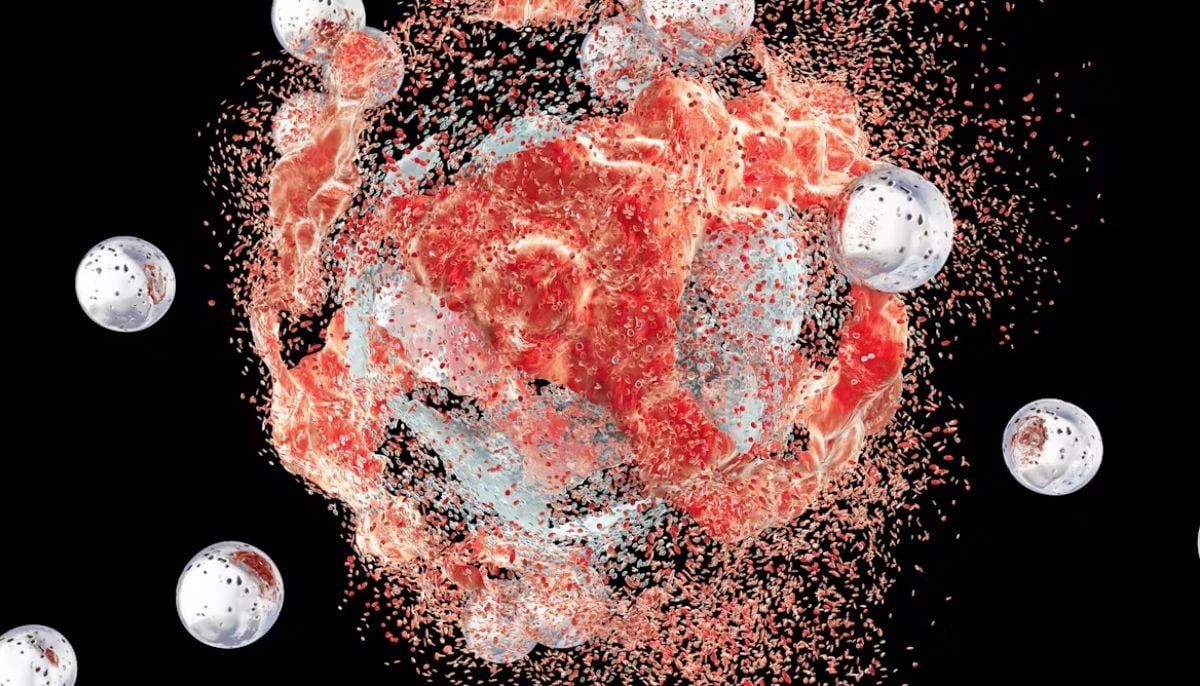
New tests could nearly halve the rate of late-stage cancers, some scientists say — is that true?
What if a single blood test could determine whether you had one of 14 types of cancer?
That’s the question posed by a study published in November in the journal Cancer. Conducted by researchers at the cancer detection-test company Exact…
Continue Reading
-
Disease Outbreak News: Middle East respiratory syndrome coronavirus – Global update – ReliefWeb
- Disease Outbreak News: Middle East respiratory syndrome coronavirus – Global update ReliefWeb
- WHO issues alert after deadly coronavirus reported in Europe Manchester Evening News
- Deadly virus detected in Europe for first time in a decade
Continue Reading
-
Obesity, Sarcopenia, Host-Related Determinants of Immunotherapy Response in NSCLC – European Medical Journal Host-Related Determinants of Immunotherapy Response
HOST-RELATED determinants of immunotherapy response in NSCLC hinge on body composition, metabolism, sex, and systemic inflammation.
Host-Related Determinants of Immunotherapy Response
Immune checkpoint inhibitors (ICIs) have transformed care…
Continue Reading
-

Synbiotics Improve Diabetes Risk Factors
A multi-species synbiotic supplement has led to measurable improvements in weight, metabolic control and cardiovascular risk markers in elderly people with type 2 diabetes, according to results from a randomised controlled trial. The findings…
Continue Reading
-

Doctors fear rising tetanus cases as vaccine rates drop
Doctors are worried about even a small uptick in the terrible infection, often called lockjaw. Symptoms, which can take three to 21 days to appear, include muscle spasms that make it difficult to breathe. As the infection takes hold, a…
Continue Reading
-
Scientist find new clue to spot mental health risk
A recent study has revealed a lead to identifying individuals at risk of developing psychotic…
Continue Reading
-

Postoperative Spine Infection Definition Reaches Consensus – European Medical Journal New Postoperative Spine Infection Definition
NEW postoperative spine infection criteria standardize diagnosis across six domains, and a microbiology standalone criterion today.
Why a Standard Definition for Postoperative Spine Infection Matters
Postoperative spine infection is a serious…
Continue Reading