
As a polio vaccination team wound their way on foot towards a row of grass-roofed houses in a small village in Inhambane province, Mozambique, a voice carried on the wind. Mixed with the sounds of children playing and a rooster calling was a…
Category: 6. Health
-

Kazakhstan Steps Up Cervical Cancer Prevention as HPV Vaccine Rollout Progresses
ASTANA – Kazakhstan has started a nationwide human papillomavirus (HPV) immunization campaign in September 2024 as part of broader efforts to curb cervical cancer, a disease that claims the lives of hundreds of thousands of women globally…
Continue Reading
-

Over 99% of Hongkongers have low immunity against ‘super flu’: researchers
More than 99 per cent of Hong Kong residents have low immunity against the new “super flu”, a team of researchers has found, as they urged the public to get vaccinated against the rapidly spreading strain.Despite the low level of immunity…Continue Reading
-

Meet Dr Happi. With $100m and a steely determination could he save the world from the next pandemic? | Global health
Winning the world’s health lottery is a lonely business in the current climate. “It’s like being an orphan in a space where there used to be many kids playing – suddenly everybody’s gone and you’re just there with a ball,” says Dr…
Continue Reading
-

Measles Outbreak Challenges States
Measles cases continue to rise amid holiday preparations and celebrations, inciting an increasing need for infection control and prevention protocols. Recently, South…
Continue Reading
-

Integrating the genome and exposome for precision health in Kuwait – News
Pedestrians cross a road amidst a severe dust storm in Kuwait City on May 23, 2022.YASSER AL-ZAYYAT/AFP via Getty Images
In the heart of the Arabian…
Continue Reading
-
Saffron as a natural modulator of reverse cholesterol transport genes in atherosclerotic rabbits, with molecular docking insights
Nedkoff, L., Briffa, T., Zemedikun, D., Herrington, S. & Wright, L. F Global trends in atherosclerotic cardiovascular disease. Clin. Ther. 45 (11), 1087–1091 (2024).
Megan, L. et al. E. LK,….
Continue Reading
-
High-Dose Rifampin Not Beneficial for Tuberculosis Meningitis
HealthDay News — No benefit of high-dose versus standard-dose rifampin is seen among adults with tuberculosis meningitis, according to a study published online Dec. 17 in the New England Journal of…
Continue Reading
-
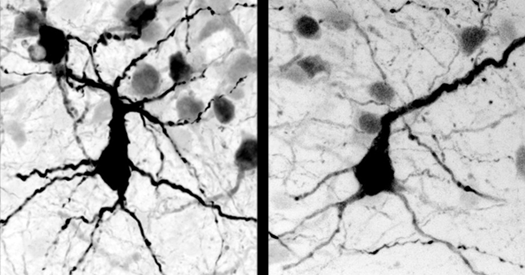
Autism in Kenya, organoid research, and more
Autism in Kenya, organoid research: In this week’s roundup, check out several papers on autism-linked genes, including PTEN, MECP2 and SYNGAP1. The list also includes a new paper documenting the prevalence of neurodevelopmental…
Continue Reading