Introduction
The global prevalence of diabetes mellitus (DM) has continued to rise in recent years, posing a significant public health concern. According to the latest estimates from the International Diabetes Federation (IDF Diabetes Atlas,…
The global prevalence of diabetes mellitus (DM) has continued to rise in recent years, posing a significant public health concern. According to the latest estimates from the International Diabetes Federation (IDF Diabetes Atlas,…

We often underestimate how much our morning rituals can set the tone for the rest of the day. When you prioritize activities that spark a natural dopamine release, you aren’t just waking up — you’re essentially giving your brain a head start on…
One of the biggest risk factors for developing liver cancer is a high-fat diet. A new study from MIT reveals how a fatty diet rewires liver cells and makes them more prone to becoming cancerous.
The researchers found that…

Canada lost its measles elimination status on November 10, 2025, after more than 12 months of sustained transmission of the highly contagious and deadly viral disease. The decision by the Pan American Health Organization (PAHO) – which is the…
This 3D illustration shows tau proteins (orange on left), which play an essential role in cells but can aggregate (orange C-shaped tubes at center and right), forming harmful deposits in the brain and causing…
Women with severe coronary heart disease causing narrowing or blockages in the arteries may derive greater long-term benefits from coronary artery bypass grafting compared with percutaneous coronary intervention, also known as…

A LARGE nationwide French cohort study has found that robot-assisted radical prostatectomy (RARP) is associated with significantly fewer short-term postoperative complications compared with both open and laparoscopic approaches. The findings…

People with HIV on antiretroviral therapy (ART) still face elevated risks of community-acquired pneumonia and herpes zoster, particularly when immune recovery remains incomplete, according to a large…
Happy holidays! I have never needed a break more than I do after this year, so YLE will be off for the next two weeks.
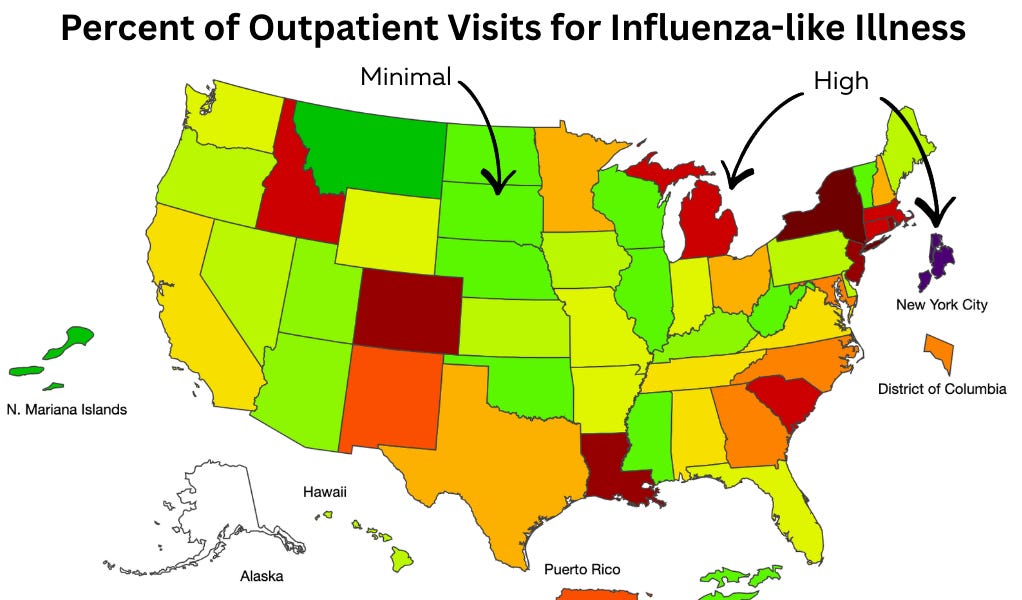
Since it’s a holiday week, this Dose was supposed to be a light one, with a quick infectious disease “weather report” to…