NIRSEVIMAB was linked to fewer respiratory syncytial virus (RSV) hospitalizations and severe neonatal outcomes than maternal vaccination with the RSV prefusion F protein (RSVpreF) vaccination in France.
RSV Hospitalization Risk Was Lower
A…

NIRSEVIMAB was linked to fewer respiratory syncytial virus (RSV) hospitalizations and severe neonatal outcomes than maternal vaccination with the RSV prefusion F protein (RSVpreF) vaccination in France.
A…

A woman said doctors dismissed her health symptoms, which included extreme fatigue, hair loss and lumps on her neck, for being a “busy mom”
She later received a shocking diagnosis and had to get a gland removed
“I knew something was…
Microplastics, plastic particles smaller than 5 millimeters, can be found in land, air, and water, and have infiltrated our food chain, resulting in far-reaching health consequences for humans and nonhumans alike. In 2020, scientists…
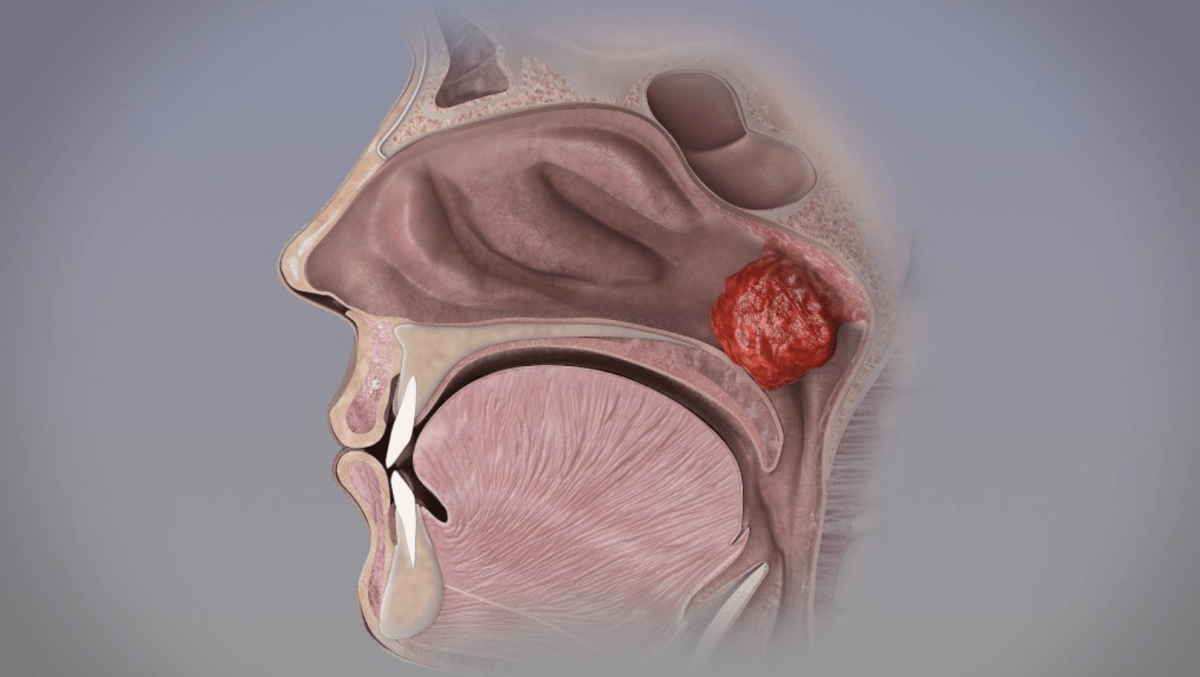
Many parents think their child’s snoring is a sign of “sleeping soundly,” but this could be a warning sign of sleep apnea. As an ear, nose, and throat (ENT) specialist, I often see parents in my clinic seeking help for their child’s developmental…

As soon as a pregnancy test comes back positive, all eyes turn to the mother-to-be: for her health and that of the unborn child, she is advised not to smoke, not to drink alcohol, to avoid certain foods, to stay calm, and not to stress out. But a…
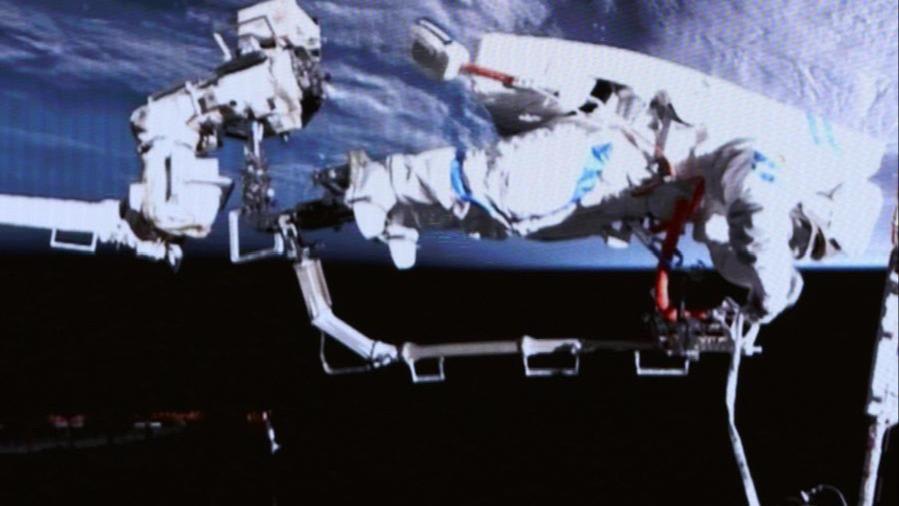
This screen image captured at Beijing Aerospace Control Center on March 16, 2026 shows Shenzhou-21 astronauts performing extravehicular activities outside China’s orbiting space station.(Photo by Zhang…

Portal hypertension (PH), a serious complication of liver cirrhosis, is defined as a pressure gradient > 5 mmHg between the portal vein and the inferior vena cava. When the hepatic venous pressure gradient (HVPG) exceeds 10 mmHg,…