Introduction
In recent years, the prevalence of type 2 diabetes mellitus (T2DM) has gradually increased, with obesity becoming a significant risk factor. Obesity, particularly visceral obesity, is closely associated with many diseases that pose…
In recent years, the prevalence of type 2 diabetes mellitus (T2DM) has gradually increased, with obesity becoming a significant risk factor. Obesity, particularly visceral obesity, is closely associated with many diseases that pose…
The coexistence of diabetes mellitus (DM) and tuberculosis (TB) resembles a “syndemic” as the two conditions intensify each other’s effects through a synergistic interaction. Individuals with T2DM have a two-to-four fold…

Posted on 22 December 2025
Image: Simon Reza, Unsplash.com.
As part of the…
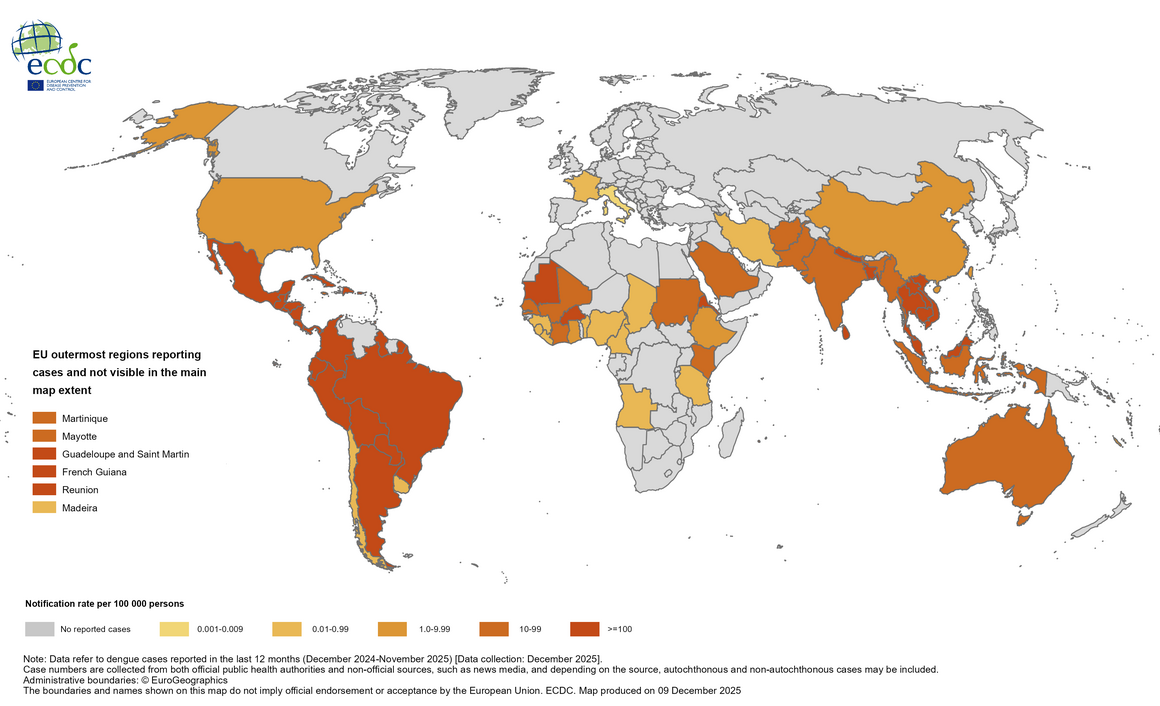
Since the beginning of 2025, and as of early December 2025, over 5 million dengue…
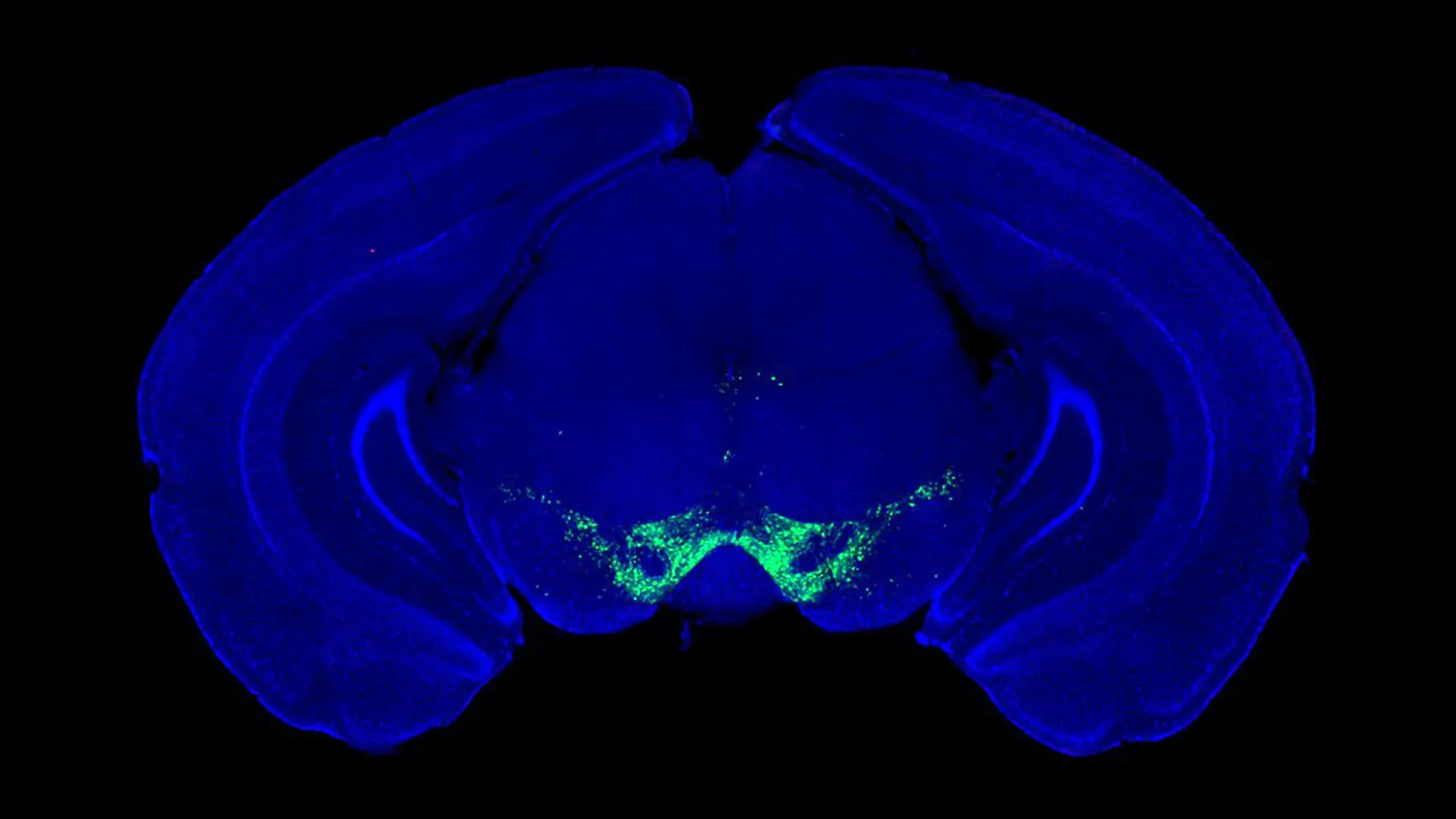
A new study led by researchers at McGill University is calling into question a long-standing idea about how dopamine influences movement. The findings suggest a shift in how scientists understand Parkinson’s disease and how its treatments work.