(Vax-Before-Travel News)
While two malaria vaccines are currently in use in Africa, a new, innovative vaccine candidate is advancing in human clinical trials. Results from a study highlight the potential of multistage vaccines to address both…
While two malaria vaccines are currently in use in Africa, a new, innovative vaccine candidate is advancing in human clinical trials. Results from a study highlight the potential of multistage vaccines to address both…

When I recently had the flu, I spent the first few days in bed coughing, sneezing and sweating off a fever. My mattress was disappearing beneath a mountain of soggy tissues, to the point where my bed was like this giant flu bomb waiting to…
Nearly half of U.S. adults — about 120 million people — have high blood pressure. That’s approximately 119.9 million Americans.
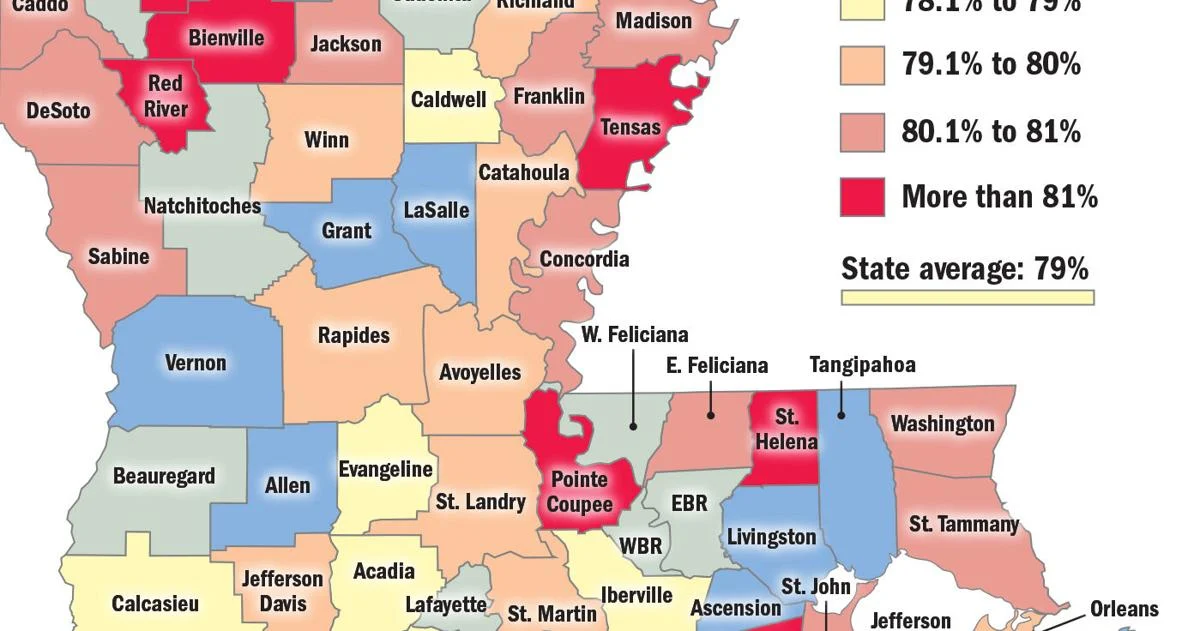
Louisiana had the fourth-highest rate of high blood pressure in the country, with 39.9% of adults reporting a…
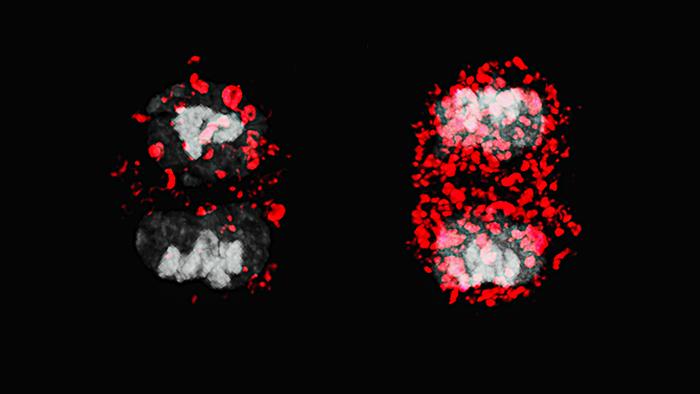
Researchers at the Max Delbrück Center and the University of Oxford have found that a cellular housekeeping function called autophagy—by which cell components are broken down and recycled—plays a major role in ensuring that T…

A NEW study used high-throughput proteomics to uncover molecular clusters and biomarkers linked to disease severity in bullous pemphigoid (BP), offering insights that could guide personalised treatment strategies.
Bullous pemphigoid is a…

December is often a time of celebration and holidays, but for some, it’s also when the cold winter weather and lack of sunlight can darken your mood.
It’s estimated that about 15 per cent of Canadians will have at least one mild episode of…
