von Braun, J., Afsana, K., Fresco, L. O. & Ali Hasan, M. H. (eds) Science and Innovations for Food Systems Transformation (Springer International Publishing, 2023); https://doi.org/10.1007/978-3-031-15703-5
Bodirsky, B. L. et al. The ongoing…
von Braun, J., Afsana, K., Fresco, L. O. & Ali Hasan, M. H. (eds) Science and Innovations for Food Systems Transformation (Springer International Publishing, 2023); https://doi.org/10.1007/978-3-031-15703-5
Bodirsky, B. L. et al. The ongoing…
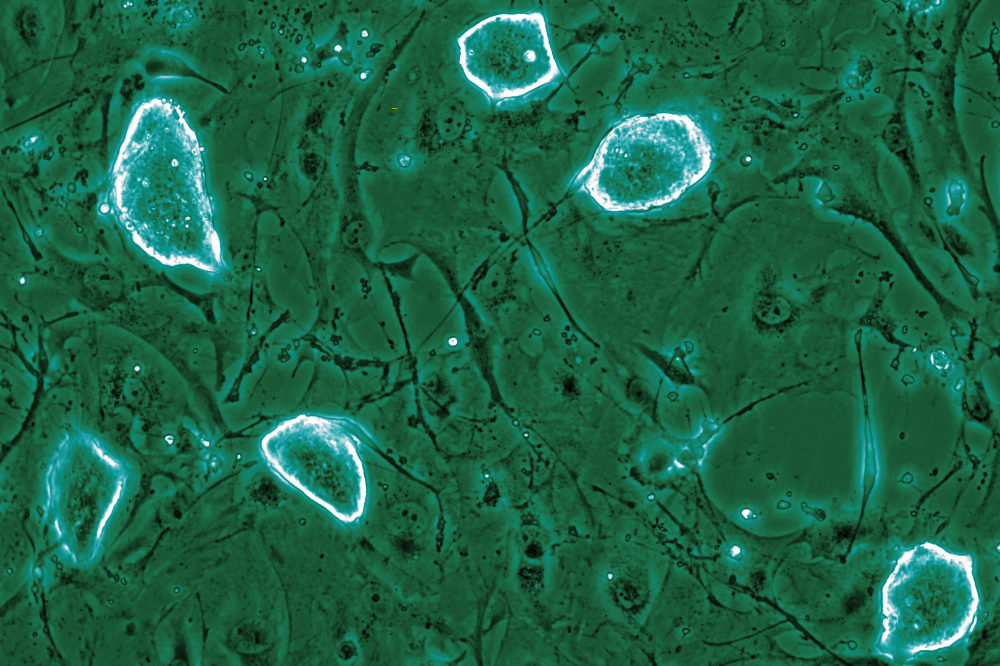
The dome shaped colonies representing diapause-like mouse embryonic stem cells. (Credit: Tarakhovsky lab)
Seals give birth only when conditions are right. After mating, a female seal can delay implantation of the embryo in the uterine…

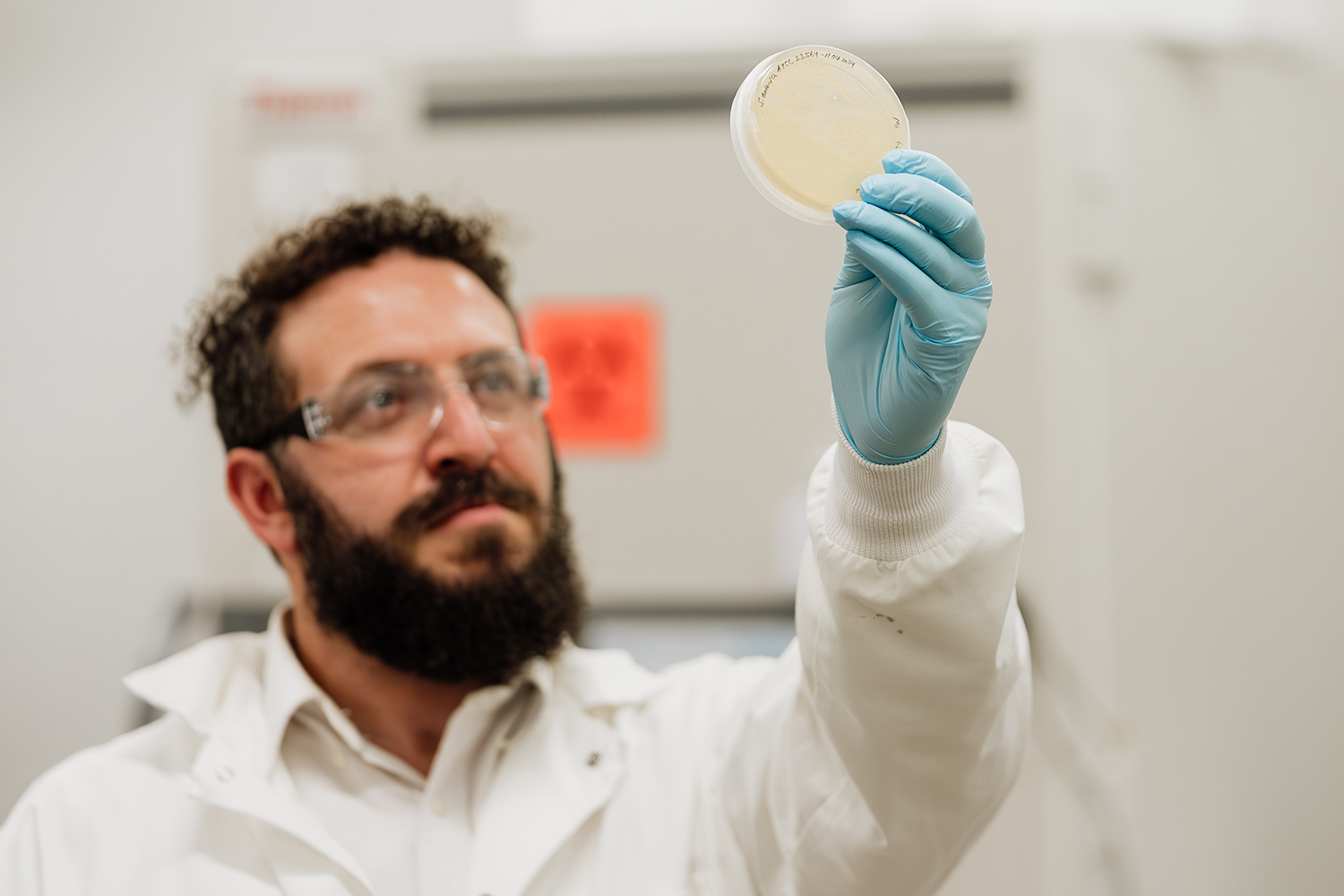
Antimicrobial resistance is on the rise, putting people’s lives on the line. According to the World Health Organization, antibiotic-resistant infections are spiking at an alarming rate, and experts predict this could lead to a

MUMBAI, India – Cervical cancer kills more than 75,000 women in India each year, according to figures recently disclosed in Parliament –…

Radiotherapy (RT) has long been a cornerstone in cancer treatment, providing local control over irradiated areas. However, recent studies have shown a phenomenon where cancer cells outside the radiation zone also regress, which…

By The ASCO Post Staff
Posted: 12/19/2025 11:00:00 AM
Last Updated:
Researchers have uncovered that sex-specific dysregulation of exosomal non-coding RNAs may drive different patterns of disease…

The Trump administration has indicated that it will fund a $1.6m study on hepatitis B vaccination of newborns in the west African country of Guinea-Bissau, where nearly one in five adults live with the virus – a move that researchers call…

As a strain of flu sweeps across the UK, experts in the Channel Islands warn it’s “something to take seriously” and are urging islanders to get vaccinated.
It comes as senior public health officials in the islands want residents to help reduce…
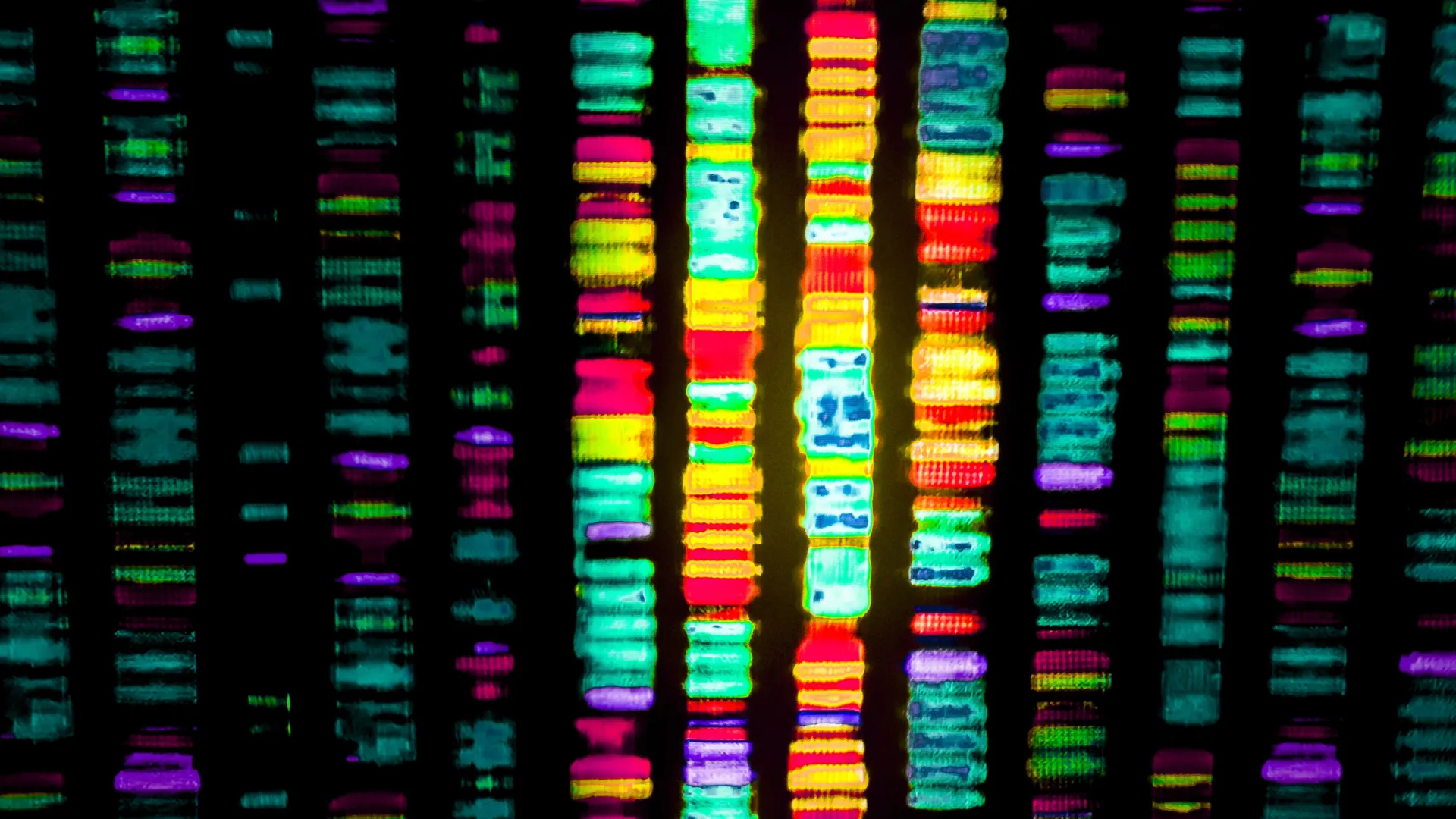
When people picture DNA, they often imagine a set of genes that shape our physical traits, influence behavior, and help keep our cells and organs functioning.
But genes make up only a small slice of our genetic code. Just around 2% of DNA…