SALIVA molecular testing showed high accuracy for pulmonary tuberculosis, clearly outperforming oral swabs in a prospective study.
Saliva Testing for Pulmonary Tuberculosis
Rapid, accurate nonsputum diagnostics remain a major need in pulmonary…

SALIVA molecular testing showed high accuracy for pulmonary tuberculosis, clearly outperforming oral swabs in a prospective study.
Rapid, accurate nonsputum diagnostics remain a major need in pulmonary…

As colorectal cancer is on the rise among people in their 20s, 30s, and 40s, a common nutrient can help reduce your risk — and you’re probably not getting enough of it.
…

IDIOPATHIC pulmonary fibrosis (IPF) progression may begin nearly a decade before symptoms, according to new modeling research.
IPF is a chronic lung disease that…

Gastrointestinal (GI) cancers represent a major global health burden and remain a leading cause of cancer-related morbidity and mortality worldwide.
Among gastrointestinal malignancies, colorectal cancer (CRC) remains one of the…

Confidential health data has been exposed online on dozens of occasions, a Guardian investigation can reveal, raising questions about the safeguarding of patient records by one of the UK’s flagship medical research projects.
UK Biobank, which…

SINGAPORE – Ms Poonam Choudhary was admitted to National University Hospital (NUH) in July 2025 following “a complete loss of physical function and troubling neurological deficits”, according to what the doctors told her.
“I had a fever,…

Irritable Bowel Syndrome (IBS) is a widespread digestive condition that affects the gastrointestinal tract. It occurs more frequently in women and commonly causes symptoms such as abdominal pain, constipation, or diarrhea. The exact cause of IBS…
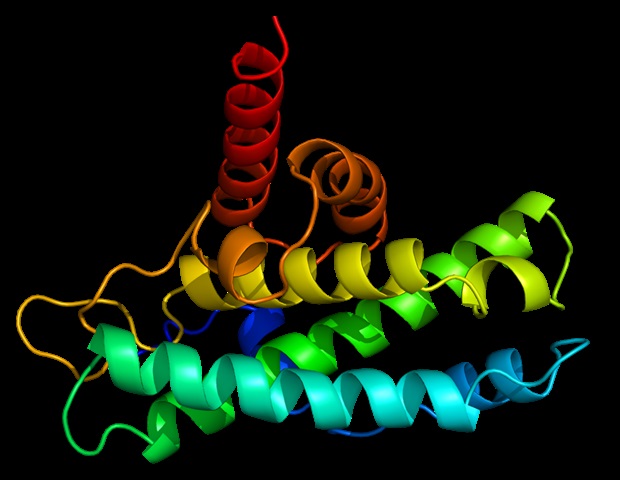
A new LMU study shows how proteins function reliably even without a stable 3D structure – and the crucial importance not only of short sequence motifs, but also of the chemical characteristics.
Many proteins do not only consist…