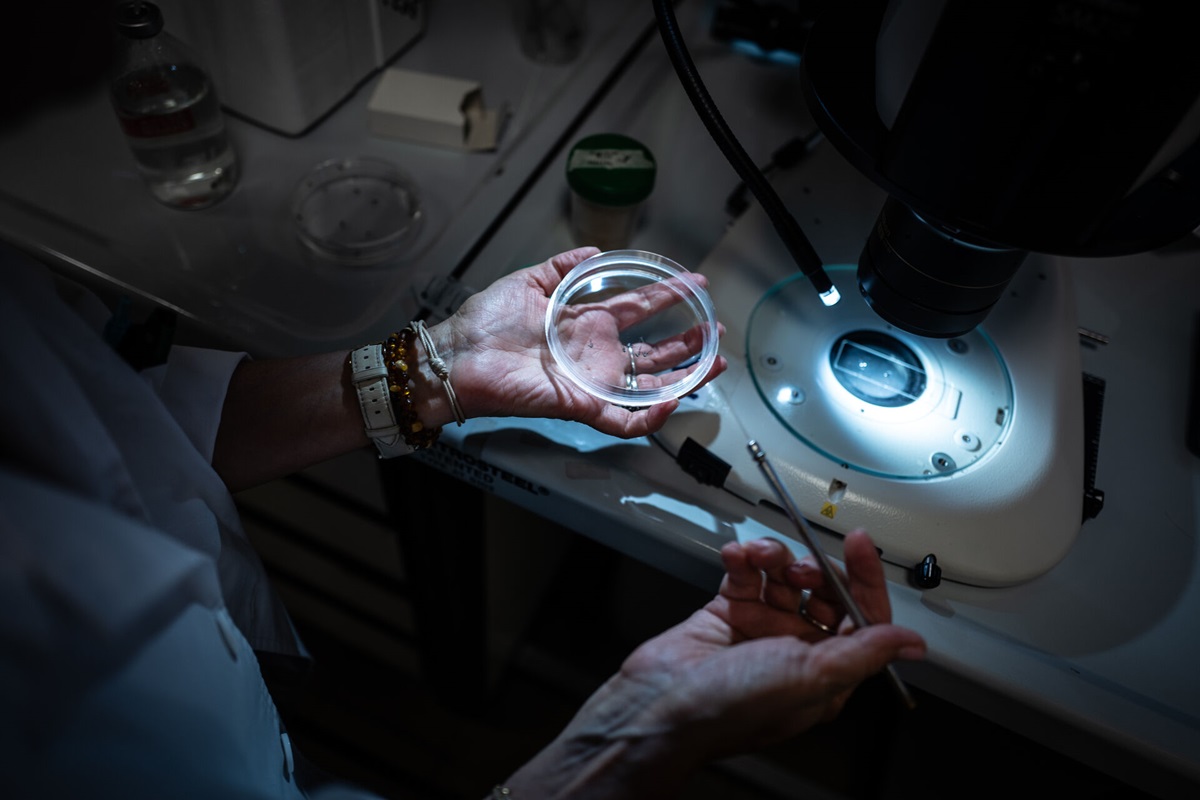
The study revealed that the smallest clusters of insulin-producing beta cells, along with single scattered cells in the pancreas, are the first to die when the immune system begins its attack. This occurs even before symptoms…
Category: 6. Health
-

Combination pills for high blood pressure may simplify treatment, improve long-term health
Statement Highlights:
- Single-pill medications that combine two or more blood pressure medications could simplify treatment to help more adults with high blood pressure achieve target blood pressure levels faster and maintain blood…
Continue Reading
-
Groundbreaking ‘preliminary’ medicine for ovarian cancer comes to light
Herbs could be the cure to ovarian cancer!
When it comes to treating this disorder, existing drugs are often limited in effectiveness and can cause…
Continue Reading
-

FDA Panelists Questioned Antidepressants in Pregnancy. But Doctors Call Them a Lifeline.
If you are pregnant or a new mother who is struggling with depression or anxiety, you can call or text the National Maternal Mental Health Hotline, 24/7: 833-TLC-MAMA (833-852-6262). Postpartum Support International can help connect you…
Continue Reading
-

How certain gut bacteria drive multiple sclerosis
Credit: AI-generated image
If gut bacteria are too similar to the protective layer of nerves, they can misdirect the immune system and cause it to…
Continue Reading
-
Cannabinoids Halt Ovarian Cancer Growth via Cell Cycle Pathway – Inside Precision Medicine
- Cannabinoids Halt Ovarian Cancer Growth via Cell Cycle Pathway Inside Precision Medicine
- Key cannabis compounds may help in the battle against one of the deadliest diseases New York Post
- Cannabis Is a Budding Strategy Against Ovarian Cancer
Continue Reading
-
WHO launches call for high-level experts to join the Science Council
The World Health Organization (WHO) is today soliciting the interest of internationally-renowned experts to serve on its Science Council, one of the Organization’s highest-level advisory bodies to the WHO Director-General.
In a rapidly evolving…
Continue Reading
-

Sex-specific associations between anthropometric indices and left vent
Introduction
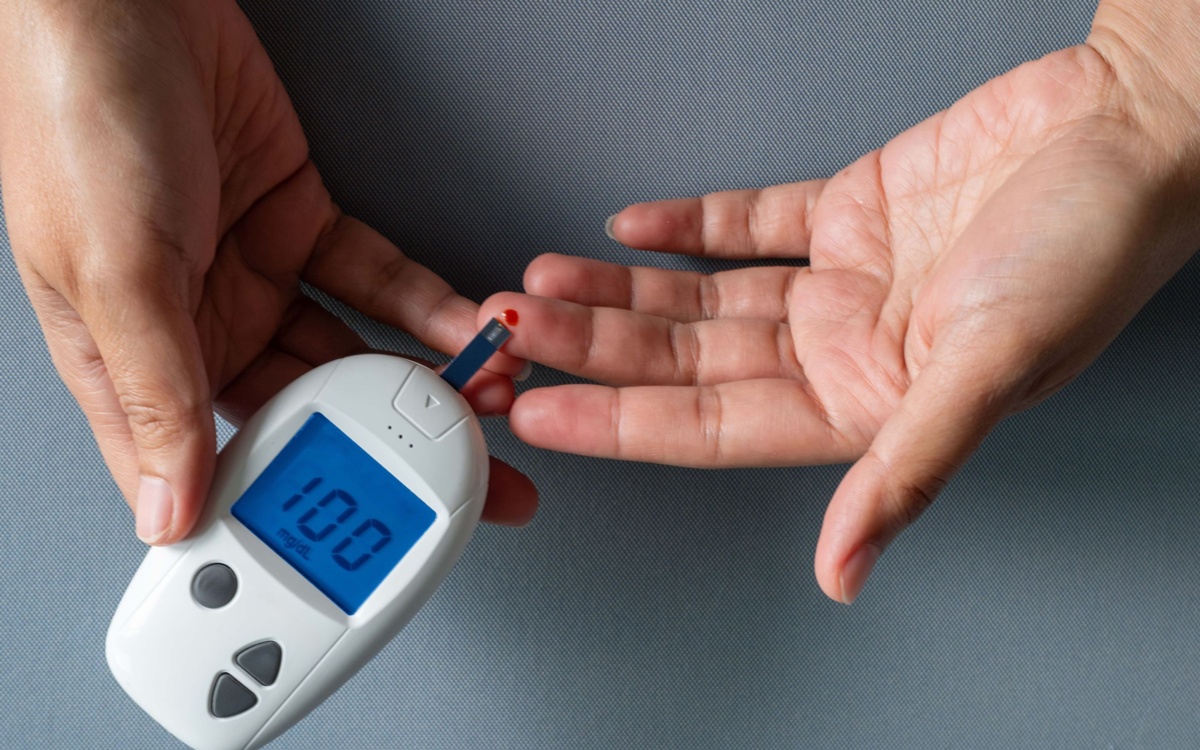
Type 2 diabetes mellitus (T2DM), a chronic metabolic disorder characterized by insulin resistance (IR) and beta-cell dysfunction, poses a significant global public health challenge. According to 11th edition of the International…
Continue Reading
-
IARC at European Liver Patients’ Association policy event at European Parliament – IARC
15 Décembre 2025
The International Agency for Research on Cancer (IARC) was represented at “From Risk to Action: Preventing Liver Health Crises through NCD Literacy and Care”, a policy event on liver…
Continue Reading
-
Dihydroartemisinin: A promising therapeutic agent against the hepatiti
Introduction
Liver cancer, especially hepatocellular carcinoma(HCC), is the fifth most common cancer worldwide and the third leading cause of cancer mortality.1 Asia is a major region for liver cancer, and Asia reported 72.5% of the world’s…
Continue Reading