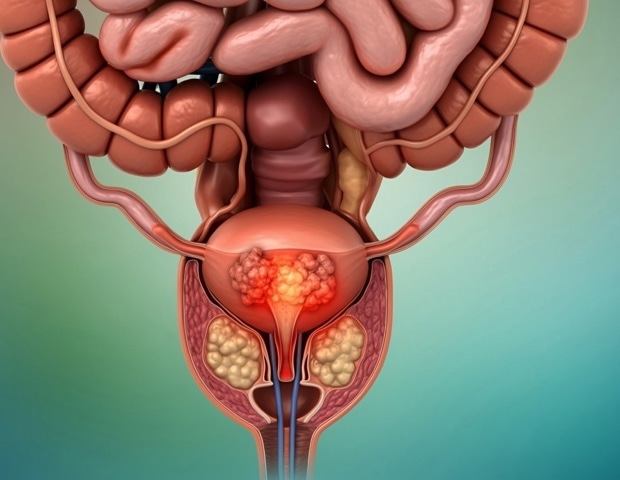
Increasing use of blood tests to detect prostate cancer is leading to overworked doctors. NTNU has now created an AI diagnostic tool that can help lighten the burden.
Diagnostic tools based on artificial intelligence are now making…
Increasing use of blood tests to detect prostate cancer is leading to overworked doctors. NTNU has now created an AI diagnostic tool that can help lighten the burden.
Diagnostic tools based on artificial intelligence are now making…

March 13, 2026
SINGAPORE – A steep rise in measles cases in Indonesia has highlighted the country’s ongoing struggle to boost immunisation rates amid growing vaccine hesitancy that has persisted since the Covid-19 pandemic.
The measles…
Clark, B. C. & Manini, T. M. What is dynapenia? Nutrition 28 (5), 495–503. https://doi.org/10.1016/j.nut.2011.12.002 (2012).
Liu, L. K., Su, Y. C., Tsai, H. C. & Chang, S. F. Dynapenic…
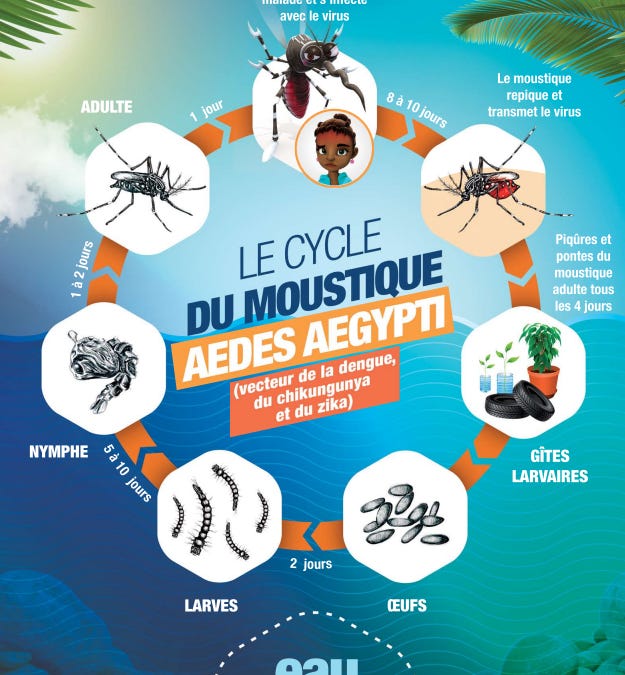
Dengue fever has returned to New Caledonia, with confirmed cases in the territory. During the rainy season, the presence of stagnant water promotes mosquito breeding and can accelerate transmission.
Since the beginning of the year through March…

iStock.com/Jacob Wackerhausen
A recent study published in the Asia-Pacific Journal of Oncology Nursing explored whether the implementation of self-management interventions could reduce cancer treatment–related cardiotoxicities among survivors of…

iStock.com/SDI Productions
Parental sense of coherence (SOC) “acts as a crucial mediator” between fear of disease progression and psychological distress among parents and caregivers of children with cancer, according to results from a recent…

The changes in the gut microbiome are registered by immune cells in the gastrointestinal tract, which spark an inflammatory response hampering the ability of the vagus nerve to signal to the hippocampus. | Image used for…
In the United States, malaria is considered by the government to be a rare disease, with nearly all cases reported in travelers returning from areas where the disease is endemic, primarily in the Americas and…

Lipid nanoparticles, or LNPs, best known as the delivery vehicle for the COVID-19 mRNA vaccines received by billions of people, are now at the center of a much larger medical revolution. Researchers are racing to use them to ferry…