The World Health Organization (WHO) published today three new Target Product Profiles (TPPs) for antibacterial agents designed to address key drug-resistant bacteria causing severe bloodstream and urinary…
Category: 6. Health
-

Training game helps nurses spot fungal infections in breastfeeding
A new educational game simulates real breastfeeding complications, helping nurses learn how to spot and manage fungal nipple infections that can cause pain and early weaning.
Study: Serious game prototype for nurses on…
Continue Reading
-
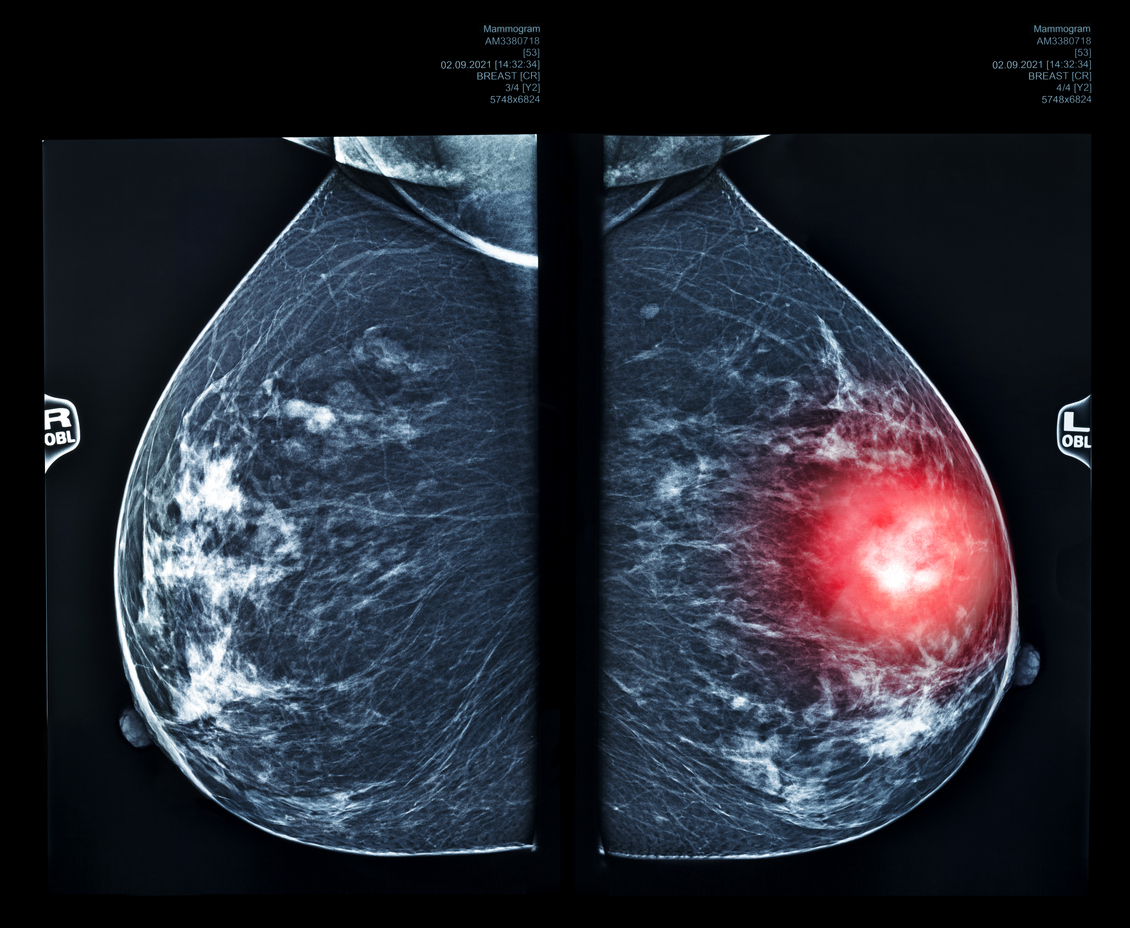
Google AI matches radiologists in detecting breast cancer in scans
Image: © SimoneN | iStock New research from Imperial College London shows Google AI can match or exceed radiologists in detecting breast cancer from mammogram scans, highlighting its potential to improve screening and…
Continue Reading
-

Rapid Socio-Environmental Shifts and Cancer Risk
North Korean defectors who resettled in South Korea share genetics but markedly contrasting early-life exposures with South Korean residents. Research published in the Journal of Internal Medicine compared overall and site-specific…
Continue Reading
-

Study Reveals Most Pandemic Viruses Jump to Humans Without Prior Adaptation
In contrast, the reemergence of H1N1 influenza A virus in 1977 was preceded by a shift in selection intensity, consistent with the hypothesis of passage in a laboratory setting.
In 1977, the H1N1 influenza A virus reemerged in humans after going…
Continue Reading
-
A longitudinal guide to early Parkinson’s progression
Critical Path Institute® (C-Path) applauds the publication of a new study in the Journal of Neurology that offers critical longitudinal insights into how symptoms and functional impacts evolve for individuals with early…
Continue Reading
-

New review reveals complex polygenic architecture underlying common epilepsies
An insightful mini-review published in Genomic Psychiatry synthesizes the rapidly expanding landscape of molecular genetic research on common epilepsies, assembling evidence from genome-wide association studies, whole-exome…
Continue Reading
-

Omega-3 fish oil supplements cut heart attacks and strokes by 43% in dialysis patients
A daily fish oil supplement may help lower the risk of serious cardiovascular complications in people undergoing dialysis for kidney failure. The finding comes from a large international clinical trial jointly led in Australia by Monash Health…
Continue Reading