Hi, it’s Jessica in New York. A White House directive is giving us insight into what could be next on RFK Jr.’s vaccine target list. More on that in a moment, but first …
Flu shots for kids may be next on the Trump administration’s…

Hi, it’s Jessica in New York. A White House directive is giving us insight into what could be next on RFK Jr.’s vaccine target list. More on that in a moment, but first …
Flu shots for kids may be next on the Trump administration’s…
Alessio Basolo, Paolo Piaggi, Valentina Angeli, Paola Fierabracci, Chiara Bologna, Edda Vignali, Daniela Troiani, Roberta Jaccheri, Caterina Pelosini, Melania Paoli, Guido Salvetti, Luca Chiovato, Jonathan Krakoff, Alberto Landi,…
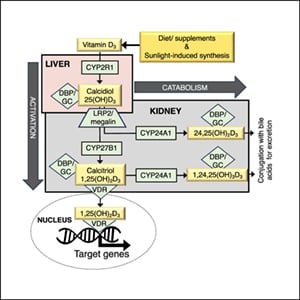
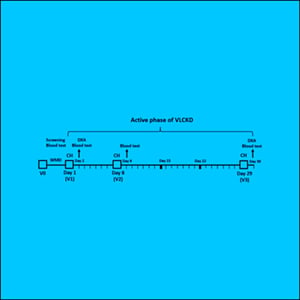
Elizabeth K Hutchins, Changran Niu, Jing Xue, Debin Wan, Carolina V Campos, Molly Warren, Megan M Knuth, Michael B Whalen, Venkata S Voruganti, Rafiou Agoro, James C Fleet, Bruce D Hammock, Folami Ideraabdullah
Endocrinology, Volume 166,…

AUTOIMMUNE diseases are associated with higher dementia risk and cognitive impairment in a nationwide Korean cohort.
Using Korean National Health Insurance Service health screening data from 2002 to 2019,…
Healthcare systems worldwide are increasingly recognised as complex adaptive systems that require leaders capable of navigating uncertainty, aligning diverse stakeholders, and sustaining high-quality service delivery despite resource…

Every year, thousands of people across Europe fall ill after eating contaminated food, with eggs, meat and ready-to-eat (RTE) food products among the most frequent sources of infection. The report shows that while food safety standards in Europe…

December 9, 2025 | Tuesday | News
CEPI is the world’s largest funder of Nipah research and development. Its $150 million portfolio—including two Nipah vaccine candidates and a monoclonal antibody—spans the whole preparedness chain, from countermeasure development and…
Pediatric drug-resistant epilepsy poses significant therapeutic challenges, with approximately 30%-40% of children failing to achieve sustained seizure free status despite the combined use of antiseizure medications (ASMs).1–3…