Updated on: Dec 08, 2025 06:09 pm IST
Category: 6. Health
-
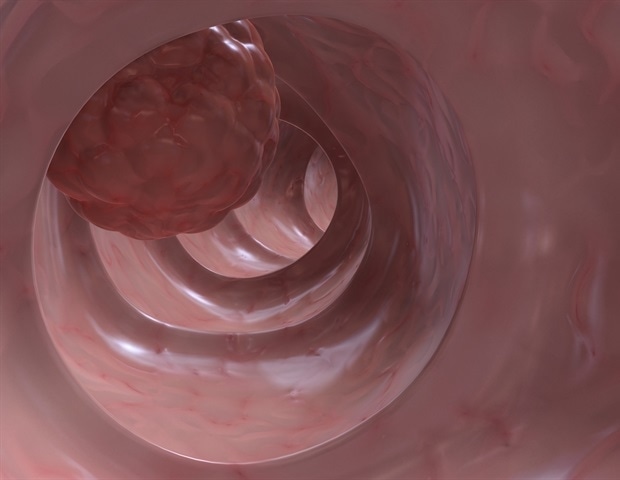
Integrating AI into colon cancer diagnosis improves the speed and accuracy of detection
A recent study reveals that integrating Artificial Intelligence (AI) into colon cancer diagnosis over the past five years has significantly improved the speed and accuracy of the detection of the deadly disease.
Published in the…
Continue Reading
-

Blood sugar migration to saliva fuels cavity development in type 2 diabetes patients
Individuals with type 2 diabetes often have a higher incidence of tooth decay, but the underlying mechanisms remain unclear. Recent evidence indicates that hyperglycemia could lead to the overwhelming presence of sugars not only in…
Continue Reading
-

Differential Causal Effects of Common Analgesics on Breast Cancer Risk
Introduction
Breast cancer remains the most common malignancy and a leading cause of cancer-related deaths among women globally, with an estimated 2.3 million new cases diagnosed annually.1 Despite advances in early detection and treatment,…
Continue Reading
-
Endocrine-Disrupting Chemicals Implicated in HS – Medscape
- Endocrine-Disrupting Chemicals Implicated in HS Medscape
- Hormone-Disrupting Chemicals from Plastics Shown to Promote a Chronic Inflammatory Skin Condition Johns Hopkins Medicine
- Toxic plastics can aggravate skin condition for Baltimore…
Continue Reading
-
Country report: ECDC Public Health Emergency Preparedness Assessment for Finland, 2024
Executive summary
Background
This assessment is based on the 16 capacities included in the template to be used by countries when providing information on their prevention, preparedness and response planning in accordance with Article 7 of the…
Continue Reading
-
New HIV Guideline Emphasizes Patient Role in PrEP Decisions – Medscape
- New HIV Guideline Emphasizes Patient Role in PrEP Decisions Medscape
- Canadian guideline on HIV pre- and postexposure prophylaxis: 2025 update CMAJ
- Student magazines are getting axed under Trump’s anti-diversity measures | As It Happens | On…
Continue Reading
-

PPARγ mediated enhanced lipid biogenesis fuels Mycobacterium tuberculosis growth in a drug-tolerant hepatocyte environment
Over the years, various anatomical and cellular environments conducive to Mtb infection have been identified, particularly concerning its latency (Cosma et al., 2003; Bussi and Gutierrez, 2019). Pulmonary TB typically presents with…
Continue Reading
-

Hydrogen Sulfide Shows Promise in Treating Nail Infections
Maintaining personal hygiene includes proper nail care, but even regular manicures and pedicures may not be enough to address nail infections once they occur.
In a recent study, scientists have discovered a…
Continue Reading