Taipei, Dec. 7 (CNA) The United States’ recent moves to scale back childhood vaccinations could create dangerous gaps in disease prevention, a former U.S. health official said, and he urged Taiwan to strengthen its diagnostic and monitoring…
Category: 6. Health
-

New Advances Transform HIV and STI Prevention
A LANDMARK new analysis highlights how rapid advances in biomedical prevention, diagnostics, and service-delivery models are transforming the global response to HIV and sexually transmitted infections (STIs). The authors report that innovation…
Continue Reading
-

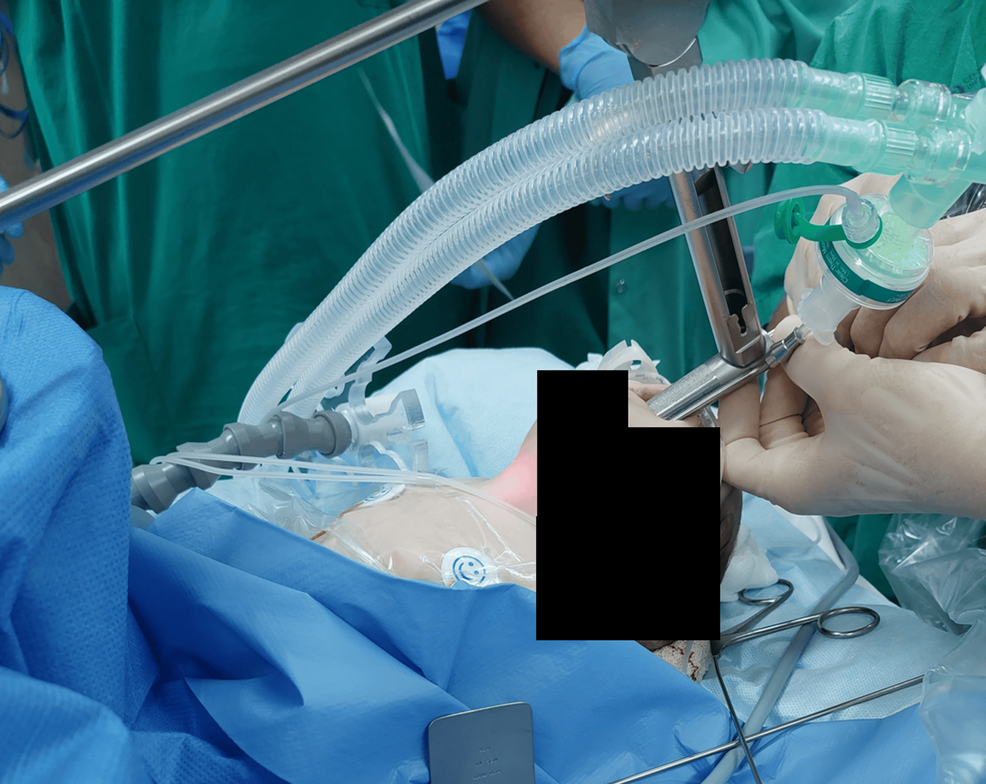
Rabid puppy found near Shoron Camp in Samaria
The Health Ministry reported a rabid puppy was discovered near Camp Horon in Samaria. 27 people who were exposed have been referred for preventive rabies treatment. The ministry further stated that “Anyone who came in contact or whose pets came…
Continue Reading
-

Namibia reports 2nd cholera outbreak of the year, the first outbreaks in more than a decade
The Namibia Ministry of Health reported six cholera cases, with three confirmed, and no deaths from Grootfontein District, Otjozondjupa Region on November 24.
This is the second cholera outbreak reported in 2025.
This year, a cumulative of 24 cases…
Continue Reading
-

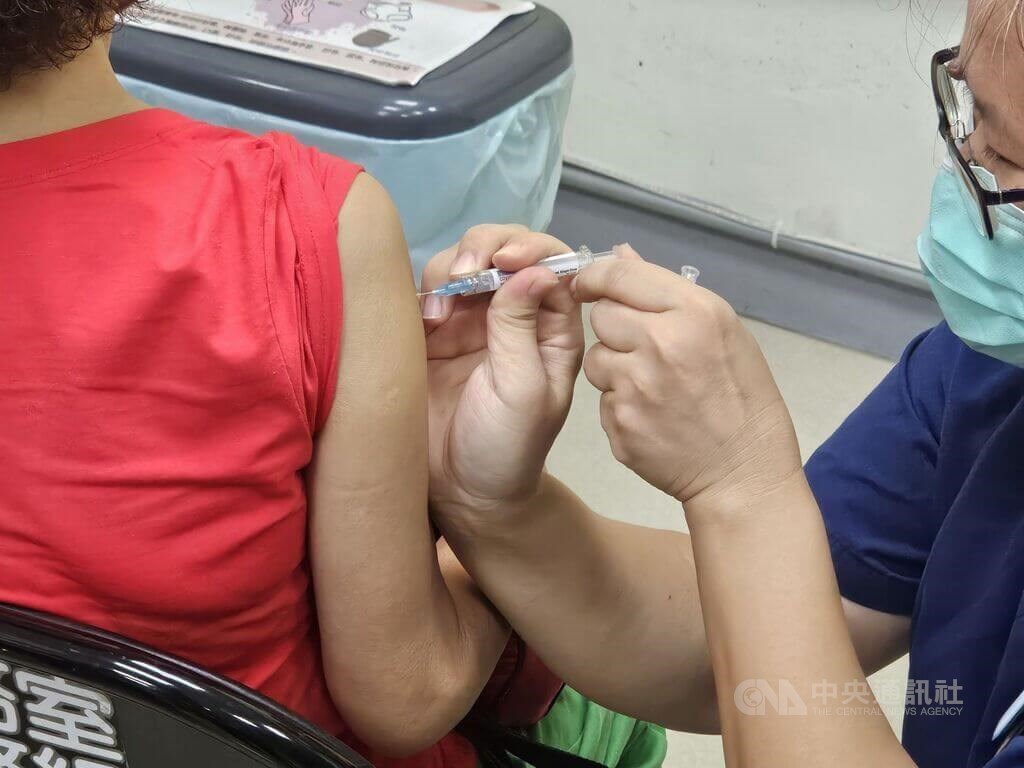
Flu cases likely to ‘spike’ in coming weeks, warns health secretary
Neil Gray spoke to BBC Scotland’s The Sunday Show about flu cases in Scotland. Flu cases in Scotland are expected to “spike” in the coming weeks, the health secretary has warned.
Neil Gray MSP said rates of the illness are following a similar trend…
Continue Reading
-
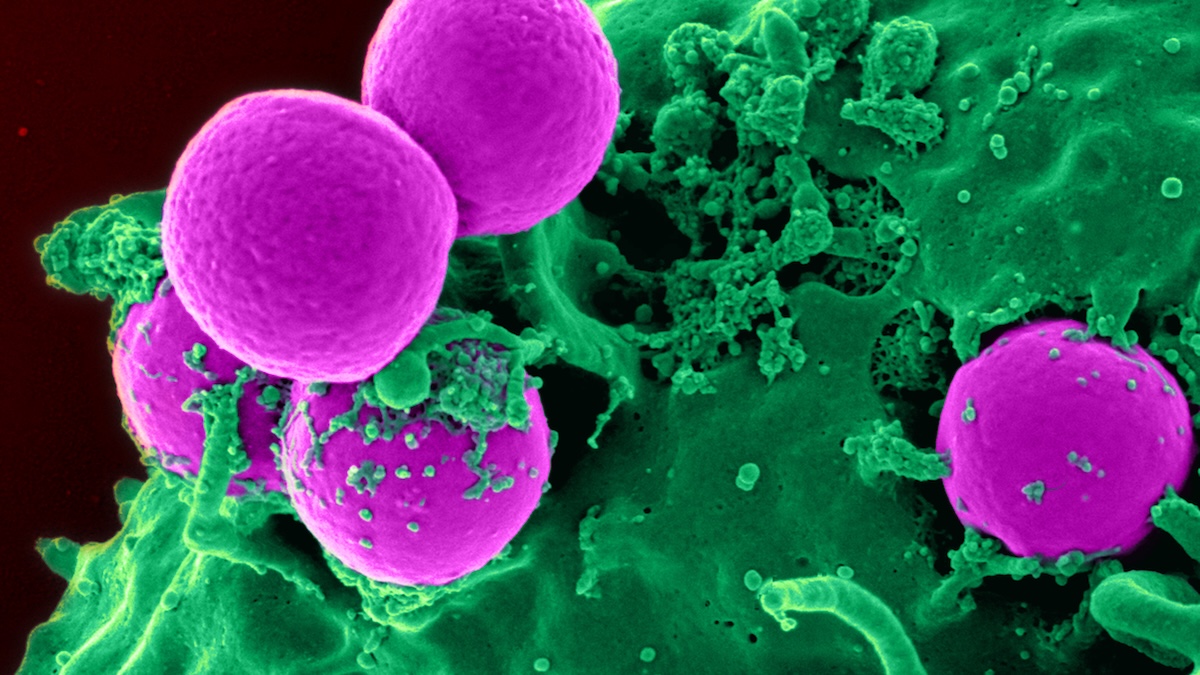
Grim Signals of Future Antimicrobial Resistance Found Lurking in Sewage : ScienceAlert
Dangerous bacteria and other disease-causing microbes are rapidly evolving ways to defy our best antibiotic medications, a phenomenon known as antimicrobial resistance. Humans are inadvertently contributing by overexposing pathogens to our…
Continue Reading
-
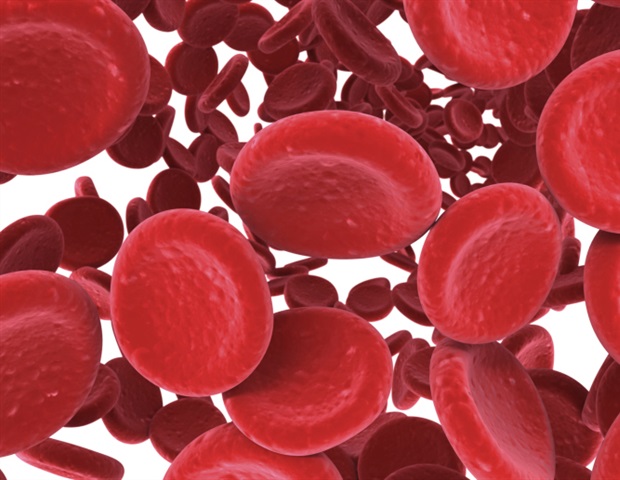
Intravenous iron shows safe and beneficial outcomes for patients with bacterial infection and anemia
Treatment with intravenous (IV) iron significantly improved survival and increased hemoglobin levels in patients with iron-deficiency anemia who were hospitalized for an acute bacterial infection, according to an analysis of data…
Continue Reading
-

Scientists keep a human alive with a genetically engineered pig liver
A recent study in the Journal of Hepatology describes the first successful auxiliary liver xenotransplant from a genetically engineered pig into a living human. The recipient survived for 171 days, providing early evidence that modified porcine…
Continue Reading