Though talks of climate change typically conjure up images of dripping glaciers and rising tides, it turns out the rapid destruction of our planet is also affecting our bodies in profound ways.
According to new research published in the journal…
Though talks of climate change typically conjure up images of dripping glaciers and rising tides, it turns out the rapid destruction of our planet is also affecting our bodies in profound ways.
According to new research published in the journal…

According to a new study published in the journal Health Psychology,…
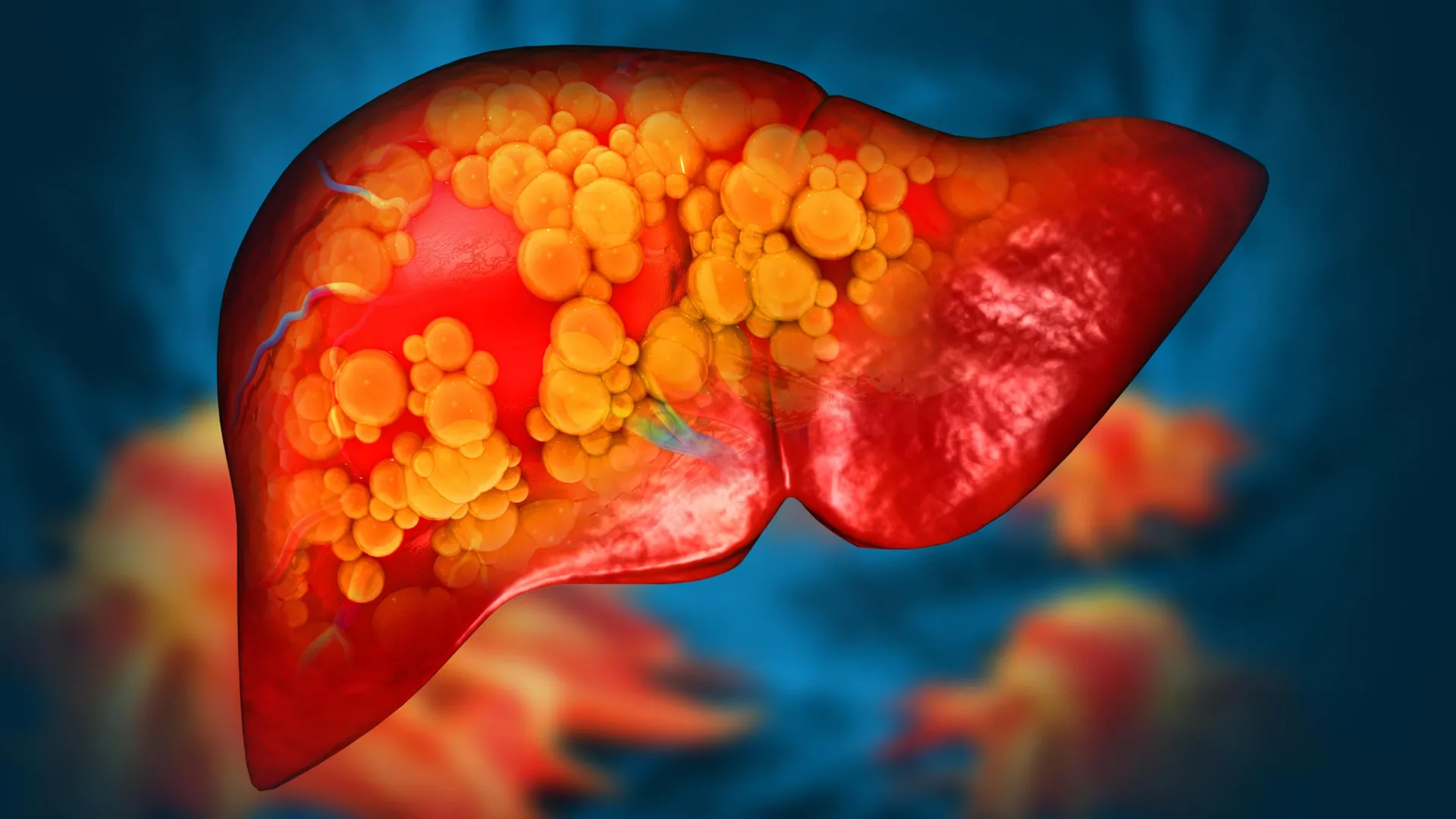
Scientists at Mayo Clinic’s Center for Individualized Medicine have identified a rare genetic variant that can directly cause metabolic dysfunction-associated steatotic liver disease, formerly known as nonalcoholic fatty liver disease.

Researchers led by scientists at UCL have discovered a protein that appears to set off diabetic retinopathy, a common eye disease caused by high blood sugar damaging the retina’s blood vessels. The condition is one of the leading causes of vision…
KABUL, March 7 (Xinhua) — Five new cases of polio were confirmed in southern Afghanistan over the past year, local broadcaster Tolo News reported on Saturday, citing the World Health Organization (WHO).
The cases were identified in…

Higher cardiorespiratory fitness linked to lower COVID-19 hospitalization risk, but not SARS-CoV-2 infection, in a large population cohort.
CARDIORESPIRATORY FITNESS is…

China”s top health official has called for greater public vigilance on cancer prevention, urging citizens to adopt healthier lifestyles and undergo regular screenings, as early detection remains critical.
Speaking at a…
With the increasing aging population, high incidence of chronic diseases, and the growing number of congenital or acquired foot deformities, lower limb dysfunction and abnormal gait problems are becoming…

Mounting evidence points to a breakdown in hospital infrastructure and management in New South Wales (NSW), with serious maintenance failures in supposedly hygienic environments now linked to preventable infections, which caused two deaths last…

Few drugs have entered mainstream awareness as quickly or as dramatically as glucagon-like peptide-1, or GLP-1 receptor agonists. Initially approved by the FDA for the treatment of type 2 diabetes, they have since also transformed…