For years, treating gum disease has meant scraping away plaque, cutting out damaged tissue or turning to antibiotics that kill bacteria indiscriminately. While newer therapies can regenerate lost tissue, doctors still lack a precise…
Category: 6. Health
-

Are socially isolated people more likely to develop cancer? Study of 350,000 adults explores the risk
A massive UK Biobank analysis suggests that objective social isolation may modestly increase cancer risk, particularly in women, highlighting how social conditions and lifestyle factors could shape long-term cancer outcomes.
Continue Reading

Sucrose reduces pain in newborns during hospital needle procedures
A new Cochrane review has found that sucrose can help with pain relief in newborn babies during common hospital procedures, such as venepuncture. This involves drawing blood with a needle, typically for testing.
Newborns,…
Continue Reading

More than 220m children will be obese by 2040 without drastic action, report warns | Obesity
Without drastic action more than 220 million children could have obesity by 2040, an international report has warned.
Globally, in 2025 about 180 million children were obese. But new figures from the World Obesity Federation suggest that by 2040,…
Continue Reading
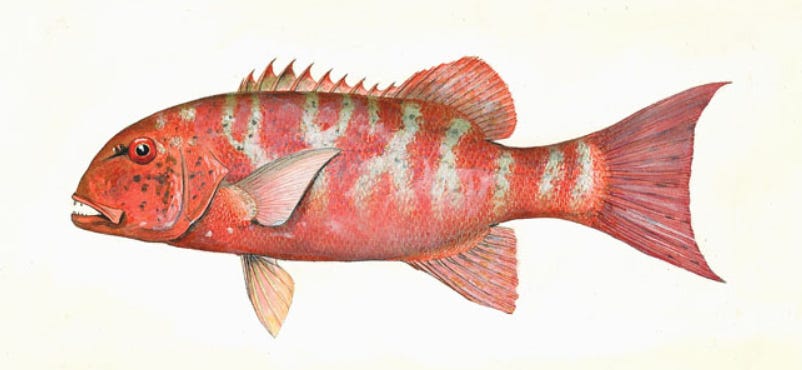
Ciguatera fish poisoning outbreak in Vanuatu
The Vanuatu Ministry of Health is reporting an outbreak of ciguatera fish poisoning. As of March 2, 44 cases have been reported between January and mid‑February 2026 across six islands (Efate, Tanna, Ambae, Pentecost, Maewo, and Santo).
No…
Continue Reading

PAHO calls for strengthened pharmacovigilance following reports of misuse of GLP-1 medicines indicated for treating obesity in adults – PAHO/WHO
Washington, DC, March 3, 2026 (PAHO) — The Pan American Health Organization (PAHO) urged countries in the Region of the Americas to strengthen monitoring and ensure the appropriate use of glucagon-like peptide-1 receptor agonist (GLP-1)…
Continue Reading
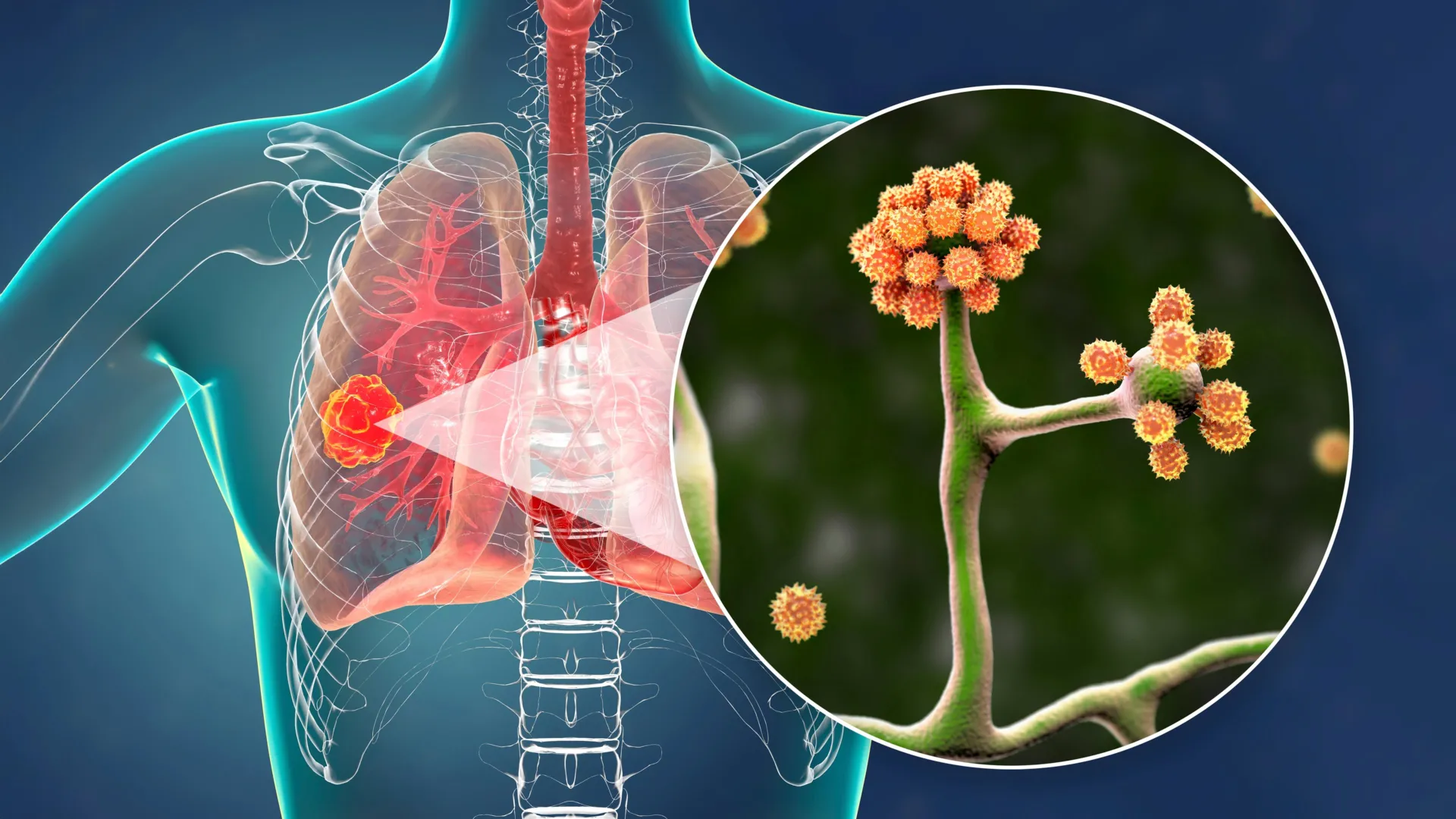
This simple blood protein could stop a deadly black fungus
An international team of scientists has discovered that albumin, the most abundant protein circulating in human blood, plays a powerful and previously unrecognized role in protecting the body from mucormycosis, a rare but frequently deadly fungal…
Continue Reading
Cerebrospinal fluid biomarkers suggest impact of herpes on brain health in people with HIV
Medscape news story
Underlying herpes infection may have an impact on brain health in people with HIV (PWH), according to new data presented at CROI 2026.
Although most PWH are also infected with herpes viruses, the impact of the resulting immune…
Continue Reading