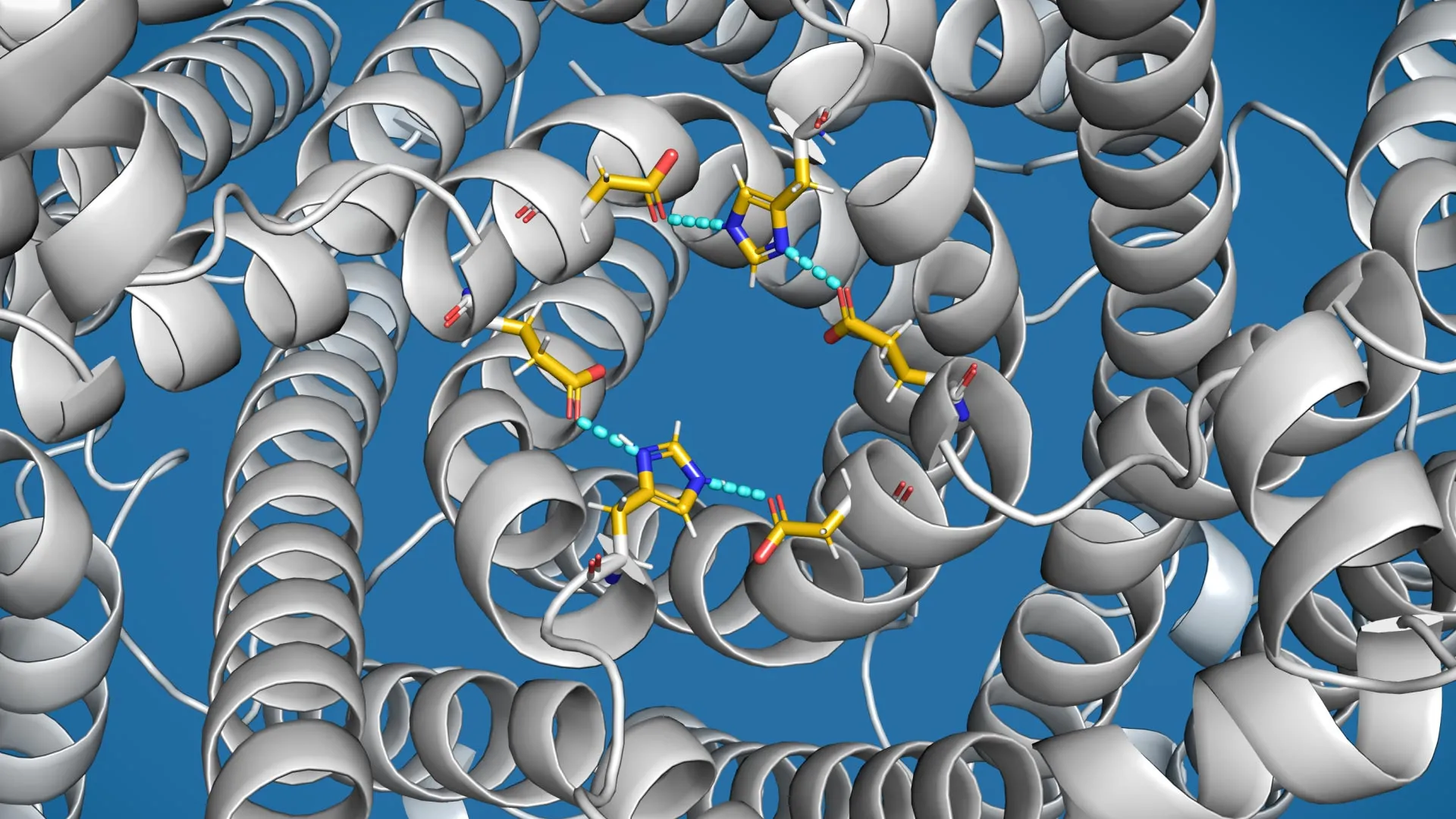
Researchers have uncovered how a mysterious ion channel helps cells break down waste, opening new possibilities for treating Parkinson’s disease.
Just like sinks and bathtubs have overflow drains to prevent spills, human cells appear to have a…
Researchers have uncovered how a mysterious ion channel helps cells break down waste, opening new possibilities for treating Parkinson’s disease.
Just like sinks and bathtubs have overflow drains to prevent spills, human cells appear to have a…
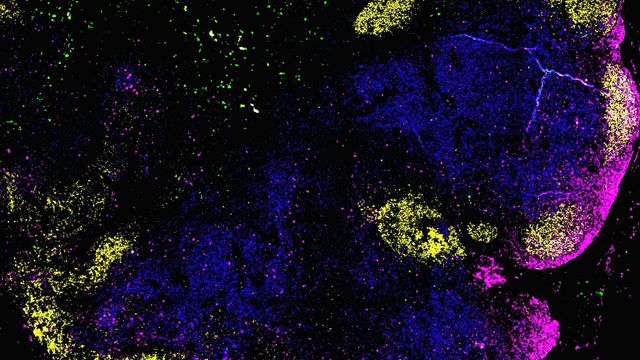
Researchers at Heinrich Heine University Düsseldorf (HHU) and Düsseldorf University Hospital (UKD) have succeeded for the first time in mapping the organization of immune cells in human lymph nodes. The study was conducted in collaboration…

Research suggests that caffeine may help restore social memory impaired by sleep deprivation by acting on one specific brain circuit that is impacted by disrupted rest. The finding offers insight into how sleep loss affects memory-related brain…

On World TB Day, 24th March, the World Health Organization (WHO) is urging countries to accelerate action to end tuberculosis (TB) and expand access to lifesaving services by using new innovations such as diagnostic tests that can be used near…

We need to see more consistent access to diagnosis, treatment, and support for people to manage their symptoms so that everyone with MS, whatever their circumstances or where they live, can live well
Catherine Godbold
The researchers also found…

Feeling like you had “a good night’s sleep” depends on more than just how long you slept. It also reflects how deeply and continuously you believe you slept. Scientists still do not fully understand what happens in the brain to create this sense…

Use of GLP-1 receptor agonists—with or without glucose-dependent insulinotropic polypeptide (GIP)—may be associated with improved clinical outcomes in patients with Type 1 diabetes, according to a large retrospective analysis published in

Human papillomavirus (HPV) is the most common sexually transmitted infection worldwide and can cause various types of cancer. Prophylactic HPV vaccination is highly effective and has been recommended in Switzerland since 2007 for…
A major new study, led by scientists at University College Dublin and the University of Edinburgh and funded by the St John of God Research Foundation, has found that commonly prescribed attention deficit hyperactivity disorder…
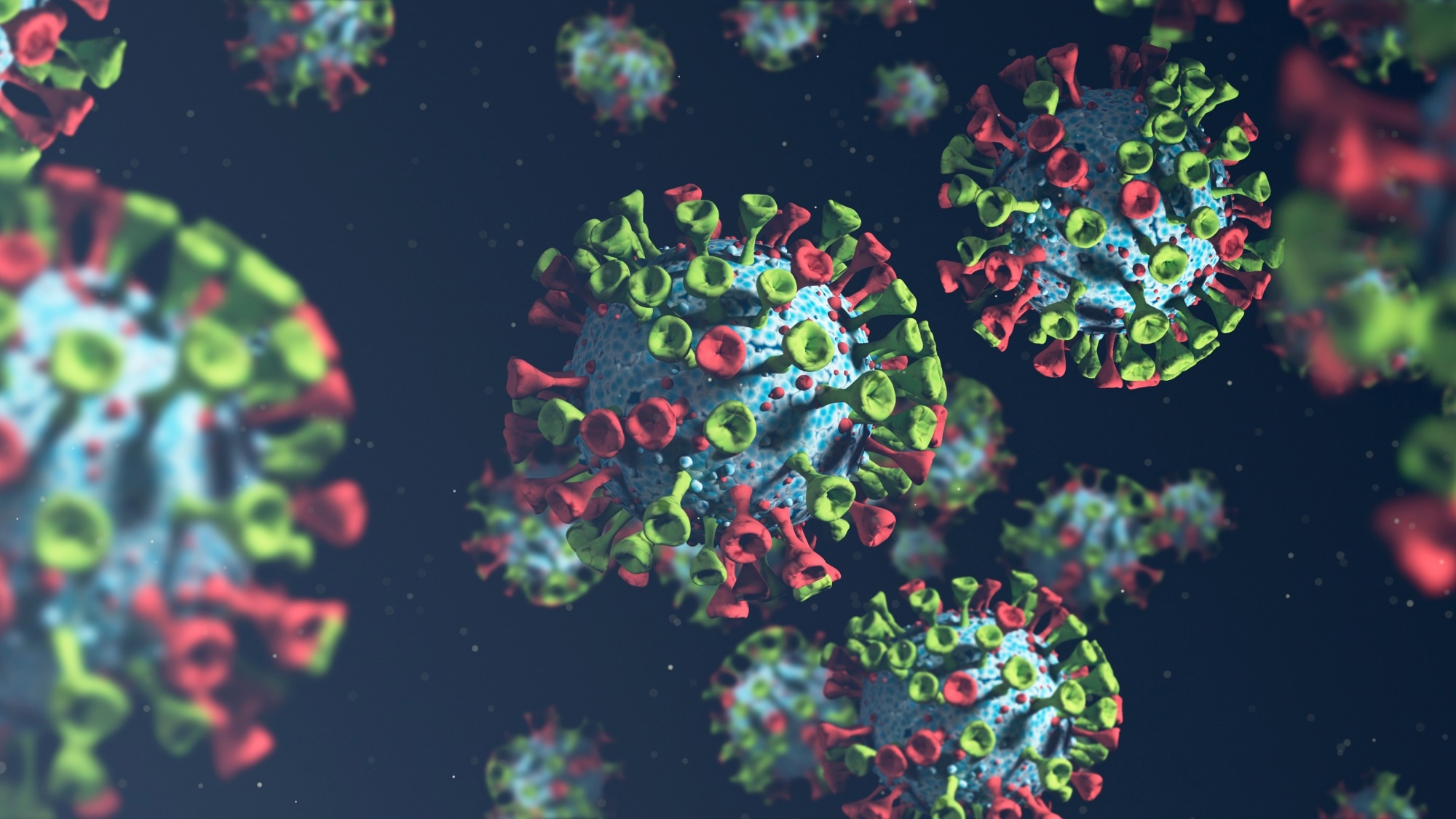
A new CDC report shows how traveler screening and wastewater monitoring detected the emerging BA.3.2 variant early, offering a clearer view of its spread, immune-evasion potential, and public health significance.
Continue Reading