Researchers at Trinity have developed a new platform for vaccine delivery they say could revolutionise treatment for respiratory infections.
Whooping cough (also known as pertussis) is a highly contagious…

Researchers at Trinity have developed a new platform for vaccine delivery they say could revolutionise treatment for respiratory infections.
Whooping cough (also known as pertussis) is a highly contagious…

NEW ORLEANS — A record-breaking 4,432 scientific abstracts accepted at the American Heart Association’s meeting here adorned posters, animated panel discussions, or drew crowds to massive halls. They promised innovations in understanding and…

A major international study involving 23,000 people has found concerning evidence about the impact of a range of common, everyday medications on the treatment outcomes for patients with breast cancer.
Led by the University of South…

A first-in-human treatment using CRISPR-Cas9 to edit the ANGPTL3 gene was well tolerated and substantially reduced both low-density lipoprotein (LDL) cholesterol and triglycerides in a phase 1 trial. The study was reported as a late-breaking…

Updated on: Nov 10, 2025 02:39 pm IST

As chronic liver disease becomes more widespread, researchers at Science Tokyo have developed a lab-grown organoid that replicates a regenerating liver, offering new hope for future treatments. The model recreates interactions between…
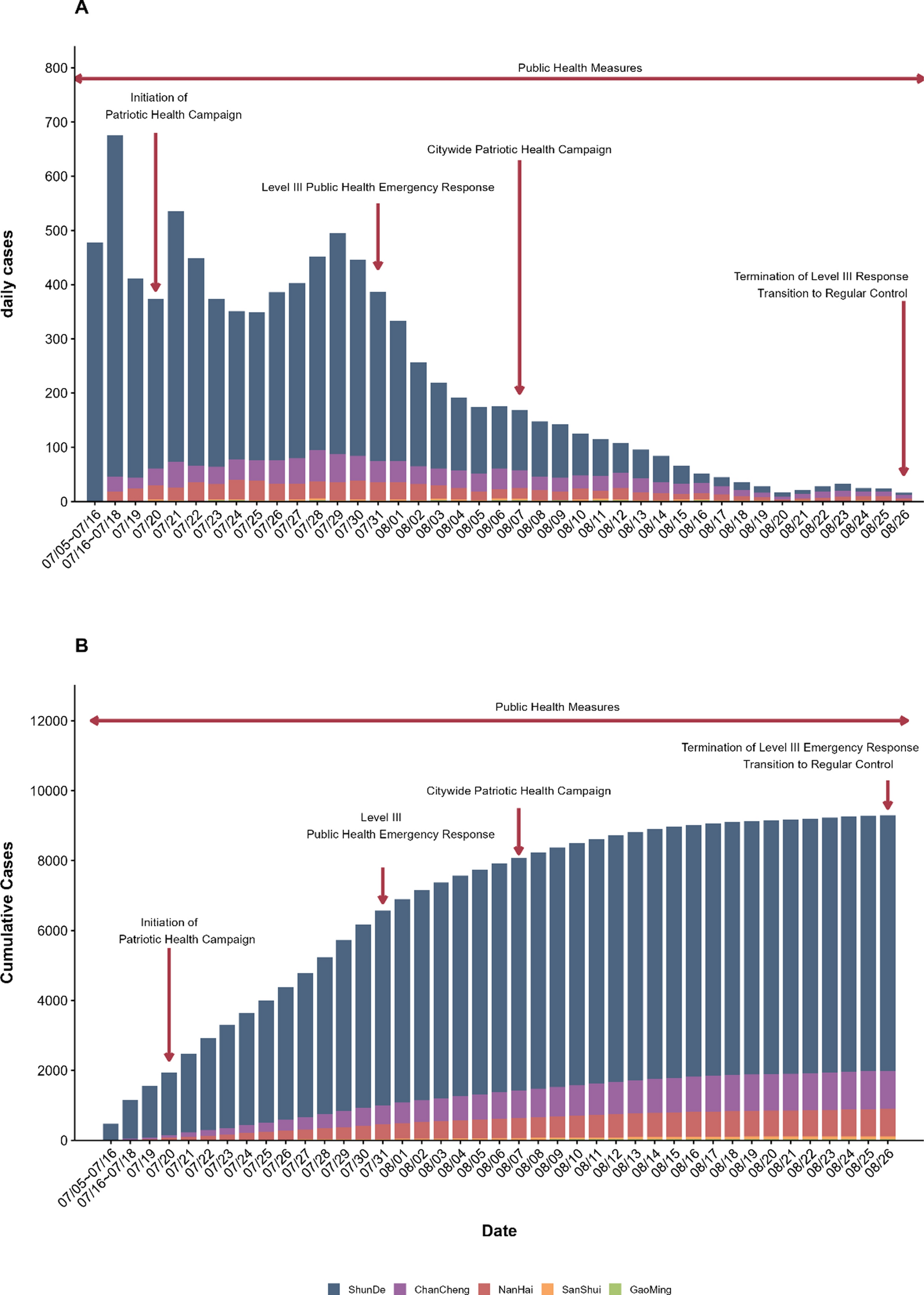
Despite successful containment, the Foshan outbreak demonstrates that post-epidemic vigilance remains critical, particularly in the context of imported-case risk and Aedes-driven seasonal resurgence, and the potential for geographic spread to…
A population of patients with borderline resectable or locally advanced pancreatic cancer who received a dose of radiation during surgery experienced disease recurrence of 5%.
Researchers at the Johns Hopkins Kimmel Cancer Center (MD,…