Patients with allergic conditions—including eczema, asthma, and hay fever—may face more problems after certain types of surgery, according to research at ACAAI 2025.
RT’s Three Key Takeaways:
- Allergic Conditions and…

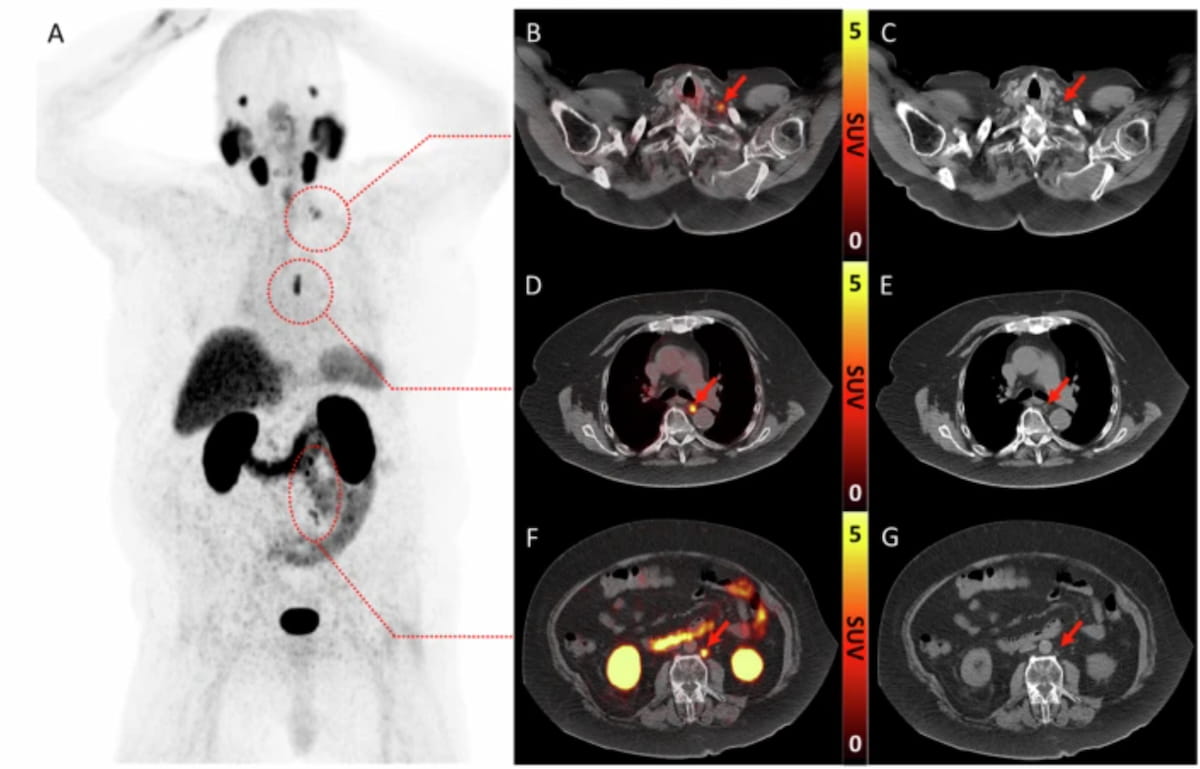
Offering current perspectives on the use of prostate-specific membrane antigen (PSMA) positron emission tomography (PET) and magnetic resonance imaging (MRI) in patients with advanced prostate cancer (PCa), the Prostate MRI Working Group of the…
Results from the phase 1 RaDDtrial (NCT03610061) radiotherapy added to immunotherapy enhanced responses, demonstrated manageable safety, and was informed by T-cell dysregulation in patients with B-cell lymphomas. 1
The objective response rate…

Use of finerenone was associated with a statistically significant 25% relative reduction in urine albumin-to-creatinine ratio compared with placebo over 6 months in patients with

About The Study: The results of this study of pharmacies in British Columbia, Canada, suggest that when medication abortion is available as a routine health service and mifepristone is regulated as a routine prescription, pharmacists…
Long-term, low doses of THC mitigate many harmful side effects and inflammation caused by HIV and antiretroviral therapy (ART), according to new research from Texas Biomedical Research Institute.
THC is short for…

MADRID – Spain will confine poultry indoors in several regions starting Nov 10 in response to escalating cases of avian influenza across Europe, the agriculture ministry said.
“Over the past weeks, we have observed an increase in the number of…
This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!

Streptococcus pyogenes or invasive Group A Streptococcus (iGAS) is a major clinical concern around the world, since iGAS infections can quickly escalate into life-threatening conditions such as necrotizing fasciitis, septic shock,…
This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!