
My boyfriend of eight years, who is 44, has ADHD and runs his own business. He’s always struggled with admin and mundane tasks, but AI has revolutionised how he works. Now I’m worried he can’t seem to do anything without AI. He is a heavy
Category: 6. Health
-

Camel Peptides Battle Drug-Resistant Bacteria
February 16, 2026—Antimicrobial resistance poses a growing global health crisis, with few new antibiotics in development. Researchers at Sultan Qaboos University have identified three novel antimicrobial peptides (AMPs) from dromedary…
Continue Reading
-
Scientists Found Cancer’s Invisibility Switch – SciTechDaily
- Scientists Found Cancer’s Invisibility Switch SciTechDaily
- Cancer Stress Protein Helps Tumors Hide from Immunity NYU Langone Health
- Mayo Clinic study identifies mechanism behind immunotherapy resistance in lung cancer Florida Hospital News and…
Continue Reading
-
New Blood Test Predicts Alzheimer’s Symptom Onset Years in Advance
A blood test that predicts Alzheimer’s onset
Researchers have identified an abnormal form of a protein called tau that circulates in the blood long before symptoms appear.
The protein, known as p-tau217, builds up in the brains of people who go…
Continue Reading
-
CD8 cell fitness predicts who benefits most from antibody-based cure strategies
aidsmap news story
Over the last few years a number of studies aiming to cure HIV or at least achieve long-term viral suppression off antiretroviral therapy (ART) have produced tantalising results. These studies have given participants one or both…
Continue Reading
-

Exercise triggers liver enzyme that repairs aging brain vessels
A liver enzyme released during exercise has recently been shown to repair aging brain blood vessels and restore memory in mice.
The new finding reframes how physical activity protects cognition by tracing its benefits to a repair process at the…
Continue Reading
-

13,000 calls in three months: How one city is keeping ahead of measles
Sometimes Lorna Grinnell-Moore, a nurse in Birmingham, gets the phone slammed down on her. Often, she has to listen to the most outlandish conspiracy theories and, on one occasion, she recalls being verbally abused.
“There’s always going to be…
Continue Reading
-
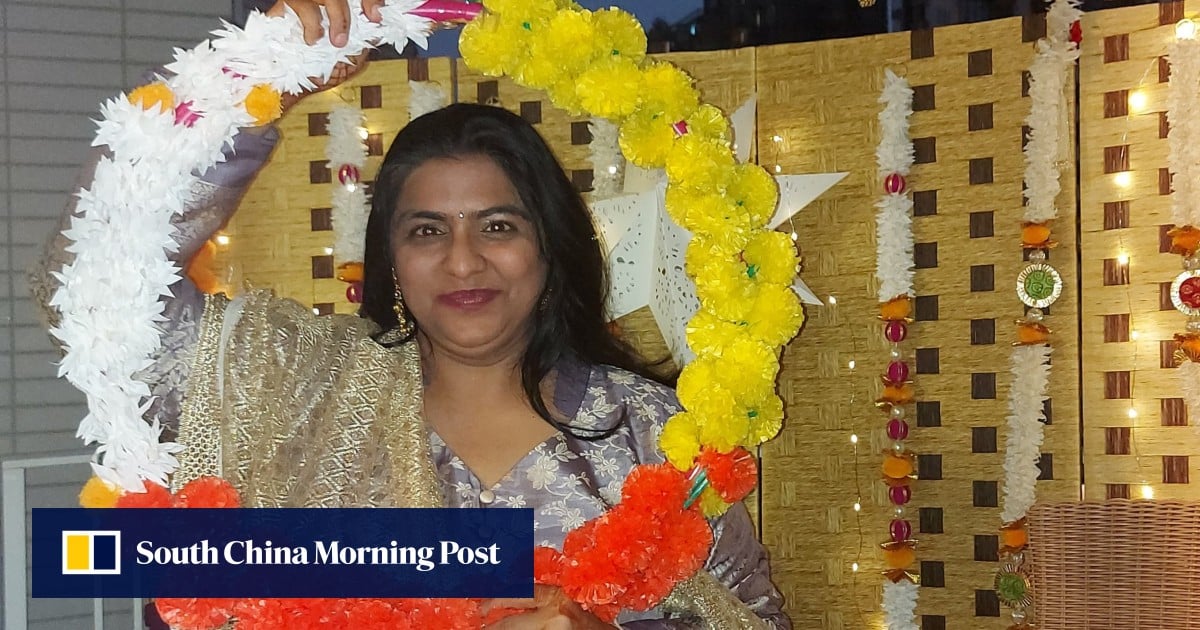
How exercise helped a mother tackle serious knee pain and return to cane-free walking
When teaching assistant Kavita Biswas first asked for a wheelchair at the airport, she was struggling to walk even short distances.
It was a world away from her active life practising yoga and dance alongside her full-time job in a Hong Kong…
Continue Reading
-
AI reads clinical notes to forecast colitis-linked colorectal cancer – Medical Xpress
- AI reads clinical notes to forecast colitis-linked colorectal cancer Medical Xpress
- AI Predicts Colorectal Cancer Risk in Ulcerative Colitis Patients National Today
- AI Technology Forecasts Colorectal Cancer Risk in Ulcerative Colitis Patients
Continue Reading
-

Study links very common food preservatives to cancer and diabetes
Food preservatives are everywhere – in sodas, packaged snacks, cured meats, and countless other staples of modern diets. For years, scientists have debated whether these additives are purely practical tools or whether some carry hidden health…
Continue Reading