- Study finds blood test can predict age of Alzheimer’s onset Fierce Biotech
- Alzheimer’s blood tests may predict when a person will develop symptoms Scientific American
- Labcorp Alzheimer’s Blood Test And Neurology Hire Spark Valuation Debate
Category: 6. Health
-
Study finds blood test can predict age of Alzheimer's onset – Fierce Biotech
-

IFN-γ identified as alzheimer’s disease blood biomarker
A new study uncovers interferon gamma as both a powerful blood-based signal of Alzheimer’s disease (AD) and a potential mechanistic bridge between genetic risk and damaging microglial inflammation in the brain.
Study:
Continue Reading
-

Scotland’s first photon-counting CT scanner set to advance multi-organ research and enhance patient diagnosis & care
The University of Edinburgh has become the first institution in Scotland to install a photon-counting CT scanner from Siemens Healthineers. NAEOTOM Alpha with Quantum Technology, joint funded by the University and British Heart…
Continue Reading
-

Fibre sources important for consumers
Summary of why fibre sources matter
- Consumers shift from fibremaxxing trends toward diverse fibre sources for health
- Different fibre types deliver distinct digestion benefits and support gut bacteria
- Soluble fibre slows sugar absorption and…
Continue Reading
-

Expert consultation for vaccine and immunization research taxonomy
WHO South-East Asia Regional Office, in
collaboration with WHO Headquarters and the Prasanna School of Public Health at
the Manipal Academy of Higher Education (MAHE), and with support from the
Wellcome Trust, developed a draft report on the…Continue Reading
-
Researchers in Australia unveil new tool for early detection of severe liver disease-Xinhua
SYDNEY, Feb. 19 (Xinhua) — Researchers in Australia have developed a new diagnostic tool that could help doctors detect serious liver disease earlier and more accurately, potentially transforming care for millions at risk.
The new…
Continue Reading
-
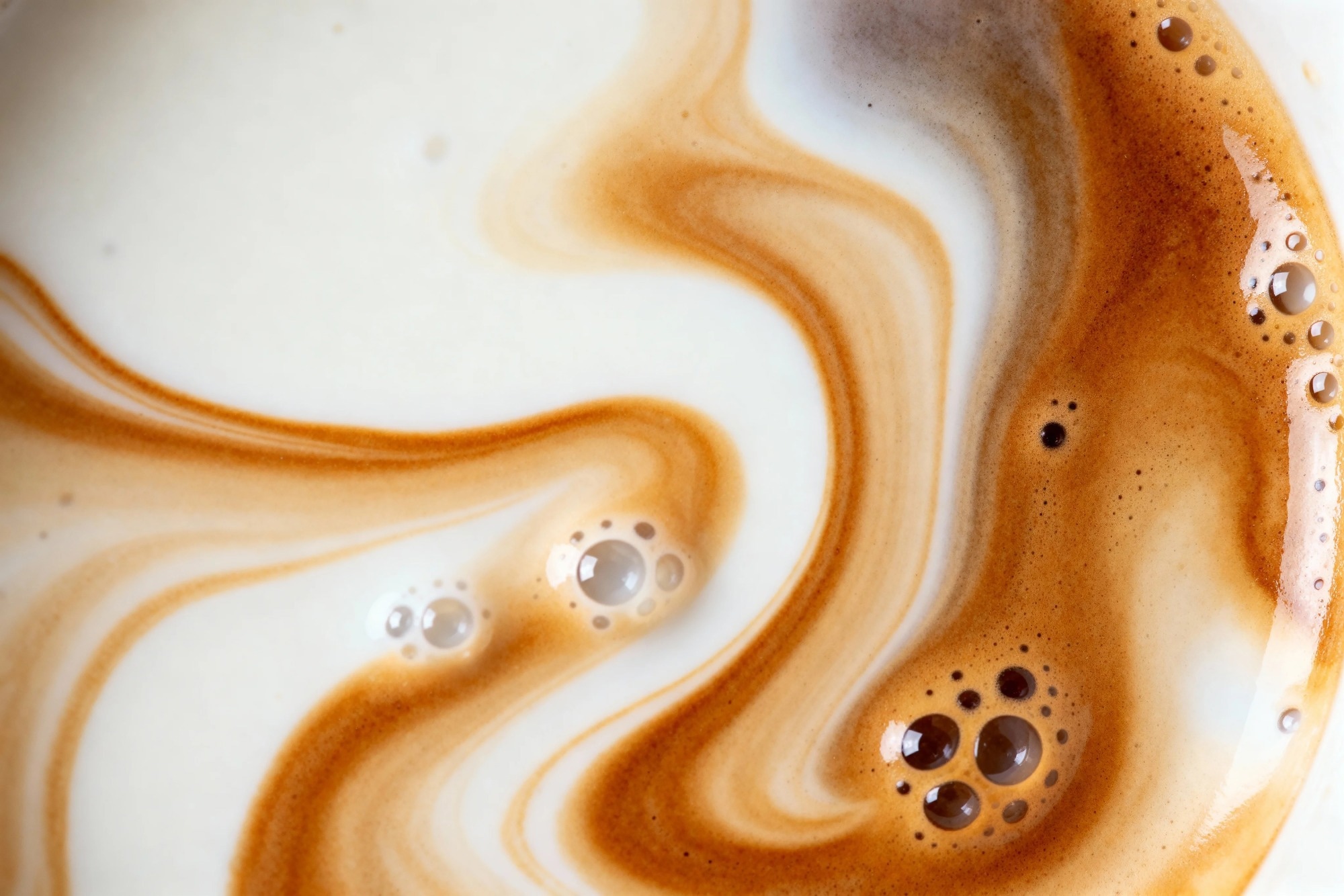
Study reveals coffee triggers distinct cytokine responses compared with pure caffeine
A controlled human study reveals that coffee’s complex chemical matrix may shape immune responses differently than pure caffeine, highlighting how everyday dietary exposures can subtly influence physiology.
Study: Immune…
Continue Reading
-
Predictive power of C-reactive protein shifts based on cirrhosis or coronary disease
A new study reveals that the predictive power of key inflammatory markers, such as C-reactive protein, shifts fundamentally depending on whether a patient suffers from cirrhosis or acute/chronic coronary disease.
Measured using an…
Continue Reading
-

Study reveals higher rates of substance use among non‑heterosexual groups in the U.S.
A study led by researchers at University of California San Diego School of Medicine reveals higher rates of substance use among all non‑heterosexual groups in the U.S., including people who are uncertain of or who use different…
Continue Reading