Qaasid News
Download Our App
Latest News from Pakistan
Pakistan opts to field in first T20 vs Sri Lanka
January 7, 2026
Taylor & Francis announces expanded scope for PeerJ journal
January 7, 2026
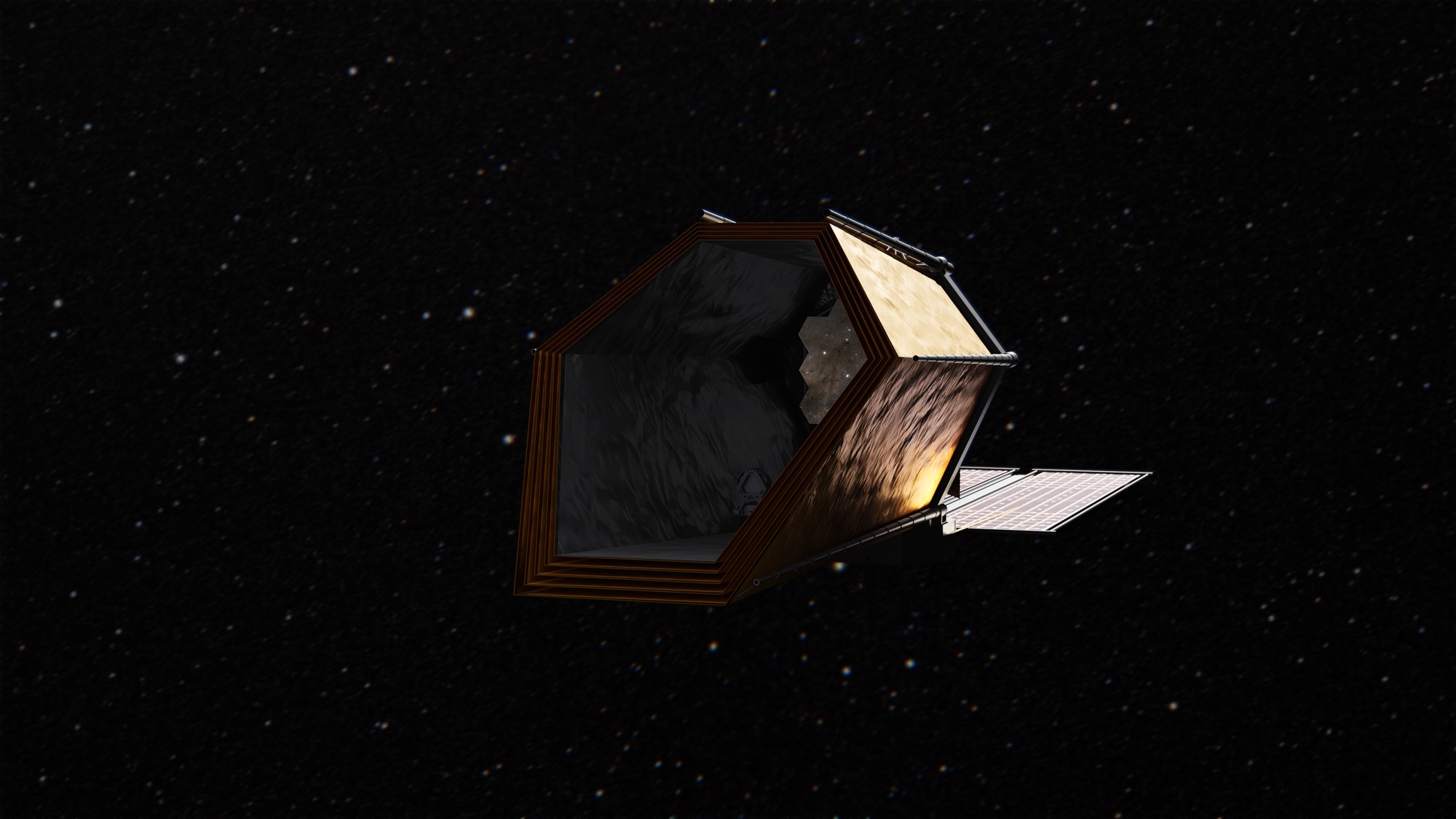
NASA seeks to accelerate development of Habitable Worlds Observatory
January 7, 2026
Classified Staff Showcase: Kenny Lipscomb | E-News
January 7, 2026
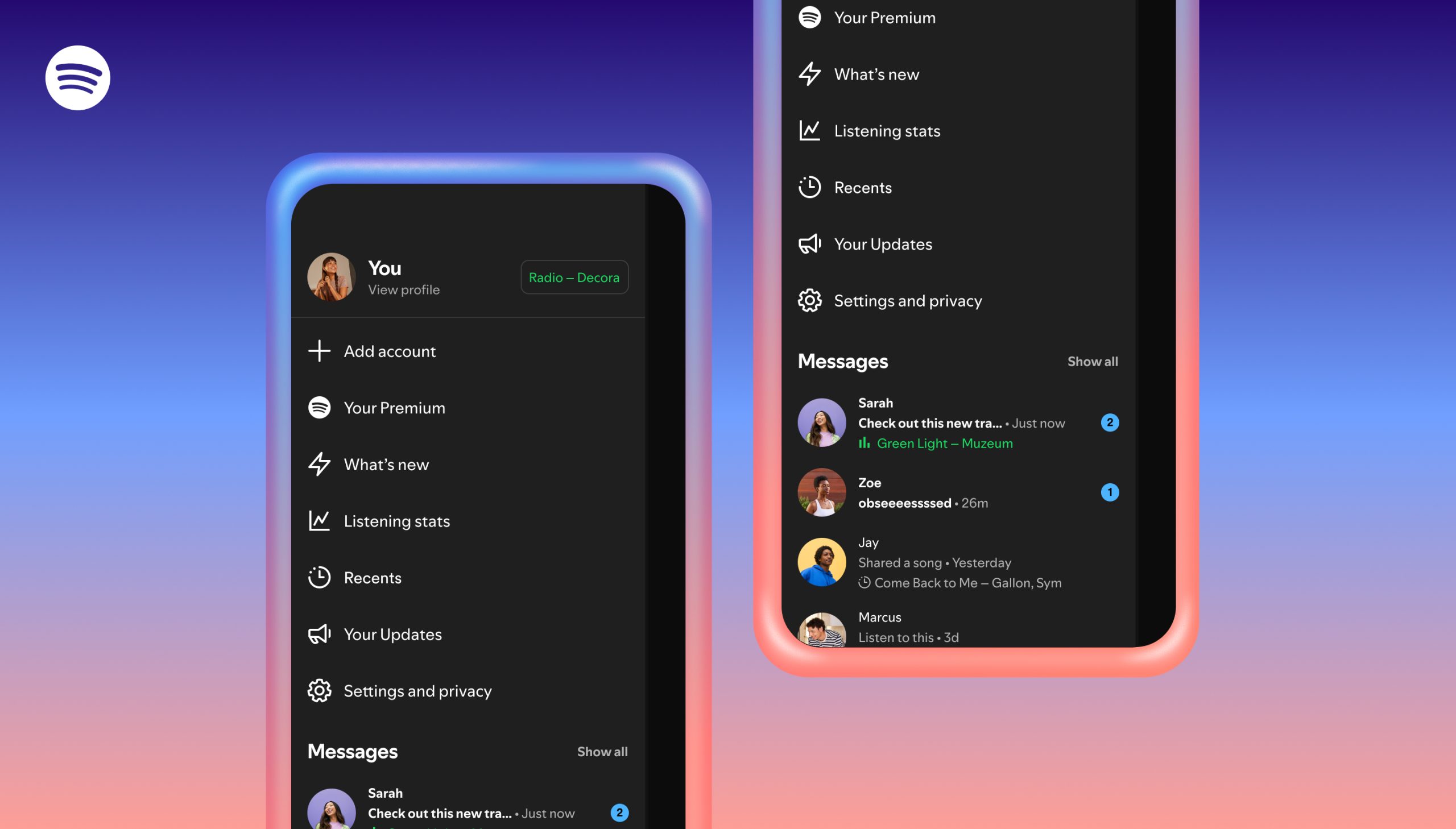
Introducing Listening Activity and Request to Jam in Messages on Spotify — Spotify
January 7, 2026
AbbVie to Host Full-Year and Fourth-Quarter 2025 Earnings Conference Call
January 7, 2026
University of Utah finds tape with only known copy of UNIX V4 hidden in storage
January 7, 2026
Oil Residues Can Travel Over 5,000 Miles on Ocean Debris, Study Finds
January 7, 2026
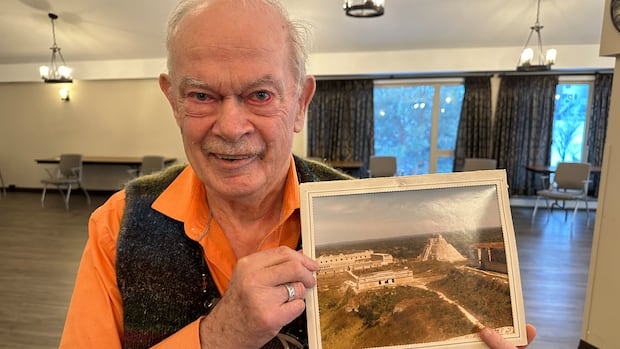
Calgary seniors’ home uses AI to turn memories into songs
January 7, 2026
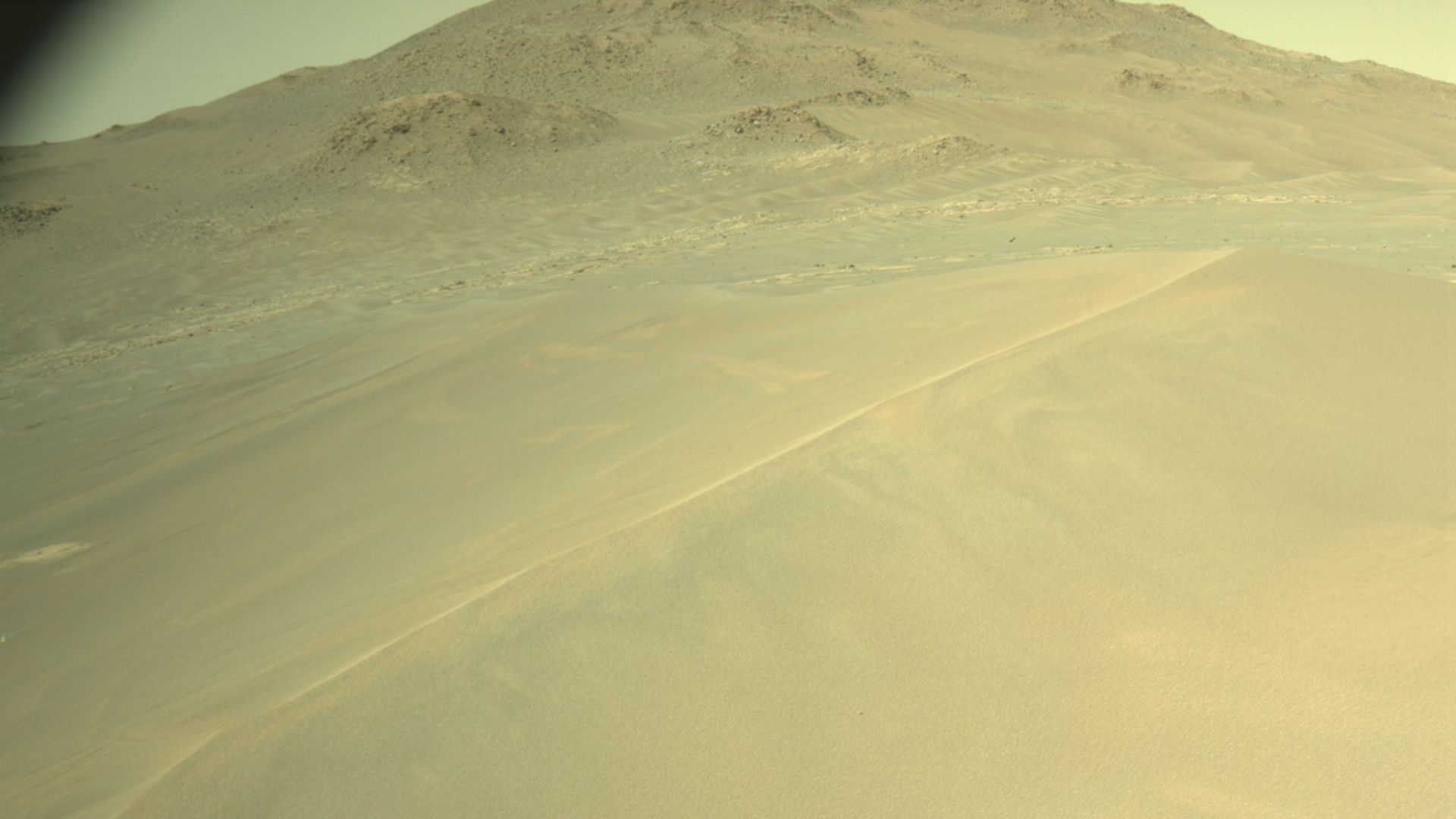
NASA Perseverance rover sees megaripples on Mars photo of the day for Jan. 7, 2026.
January 7, 2026