Qaasid News
Download Our App
Latest News from Pakistan
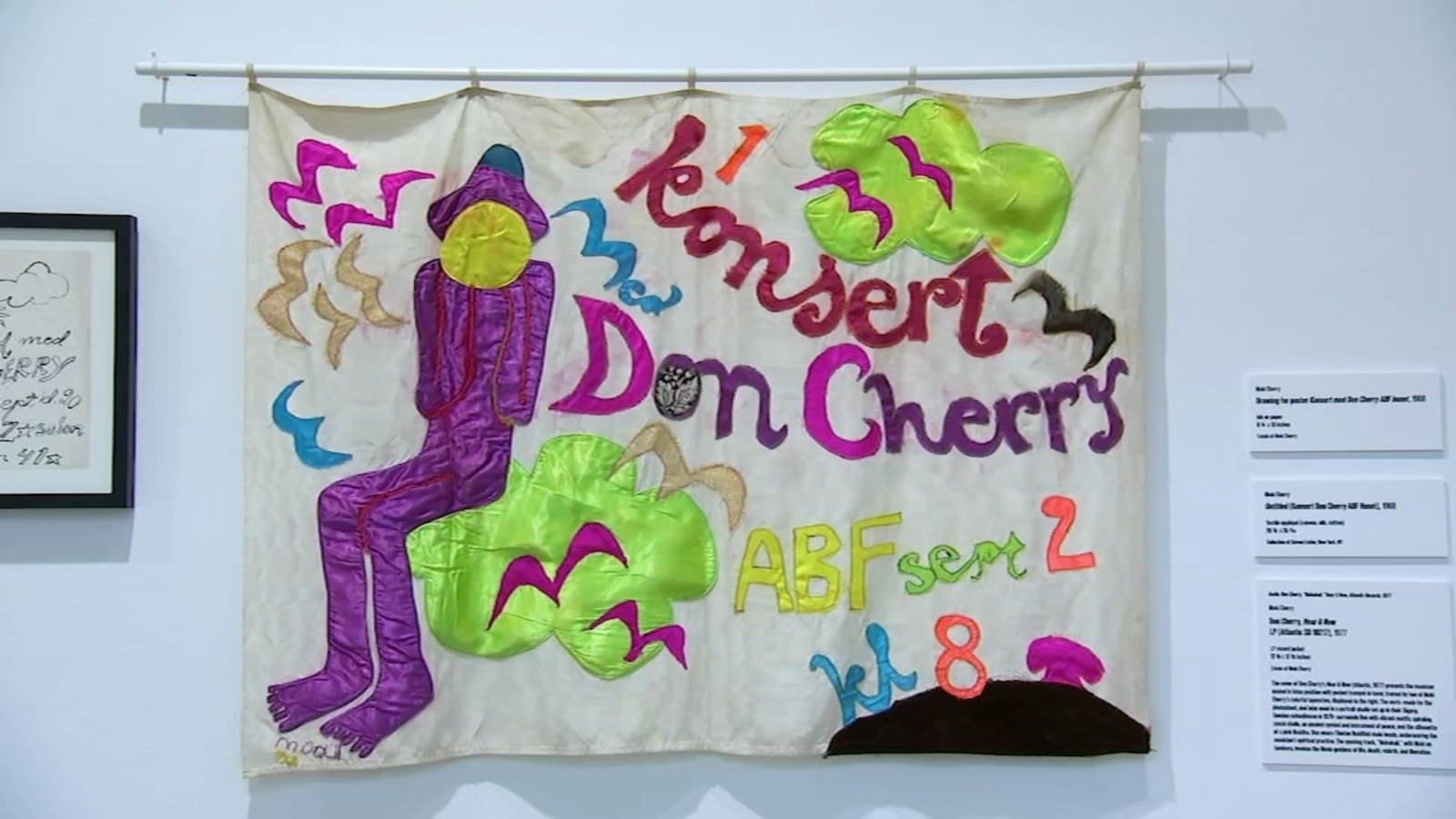
Explore Art from Moki Cherry and Lisa Alvarado at The Fabric Workshop & Museum
December 30, 2025
Telemedicine boosts coverage of HIV prevention meds
December 30, 2025
City hospital launches TMS therapy to treat neurological conditions
December 30, 2025
Robbers steal $52 million from vault of German savings bank
December 30, 2025
Carter’s Corner: A Deep Dive Into Gators’ History in Transfer Portal Era
December 30, 2025
Governor Josh Green, M.D. | DBEDT NEWS RELEASE: Visitor Spending Increased in November 2025 Despite Fewer Visitor Arrivals
December 30, 2025
Influenza Cases Surge, Raising Fears of Severe Flu Season – The Wall Street Journal
December 30, 2025
Center Times Plus, UT Southwestern
December 30, 2025
Enough fresh water is lost from continents each year to meet the needs of 280 million people. Here’s how we can combat that.
December 30, 2025
Kennedy Center renaming prompts new round of cancellations from artists
December 30, 2025