Qaasid News
Download Our App
Latest News from Pakistan
Watch Paulo Szot Perform ‘His Kiss, the Riot’ in Broadway’s Hadestown
January 20, 2026
NBA Fantasy: High Score 100 entering Week 14
January 20, 2026
India slams Poland over supporting Pakistan on Kashmir
January 20, 2026
igus 238 chainflex® cables certified for use in dry cleanrooms
January 20, 2026
Corticosteroids Associated With Development of Comorbidities in Myasthenia Gravis
January 20, 2026
Ann Demeulemeester Pre-Fall 2026 Ready to Wear Collection Review
January 20, 2026
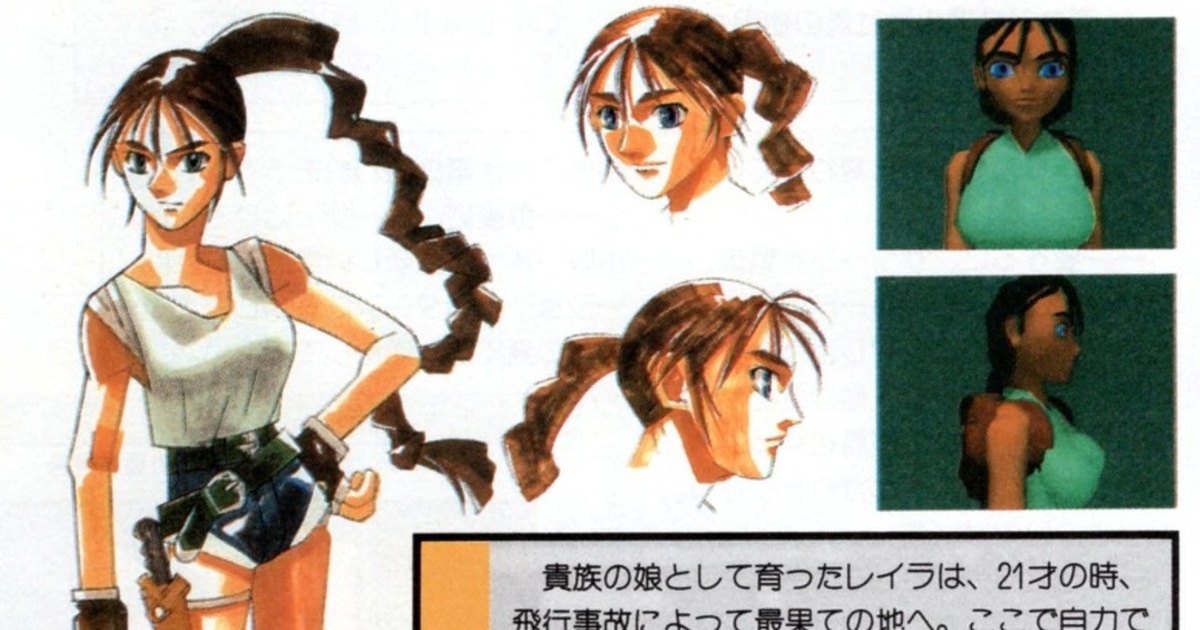
Core Design’s Japanese publisher wanted Lara Croft’s model to be changed “to appeal more to a Japanese audience”
January 20, 2026
Israel bulldozes Unrwa headquarters in East Jerusalem | Israel
January 20, 2026
Luke Mudgway wins Stage 1 in sprint finish
January 20, 2026
Salesforce (CRM) Valuation Check After Recent Share Price Weakness And Mixed Multi Year Returns
January 20, 2026