In a randomized clinical trial of older adults, researchers found that taking multivitamins for two years modestly slowed epigenetic markers of aging — equivalent to roughly four months less biological aging compared with a placebo.
Li et…

In a randomized clinical trial of older adults, researchers found that taking multivitamins for two years modestly slowed epigenetic markers of aging — equivalent to roughly four months less biological aging compared with a placebo.
Li et…
A multi-center study led by researchers at Cincinnati Children’s sheds surprising new light on why some newborns become severely ill from Escherichia coli infection, but others do not.
Turns out that most babies are immune because…
An enigmatic type of circulating tumor cell called a dual-positive (DP) cell is associated with shorter survival time in patients with advanced breast cancer, according to a study led by investigators at Weill Cornell Medicine and…
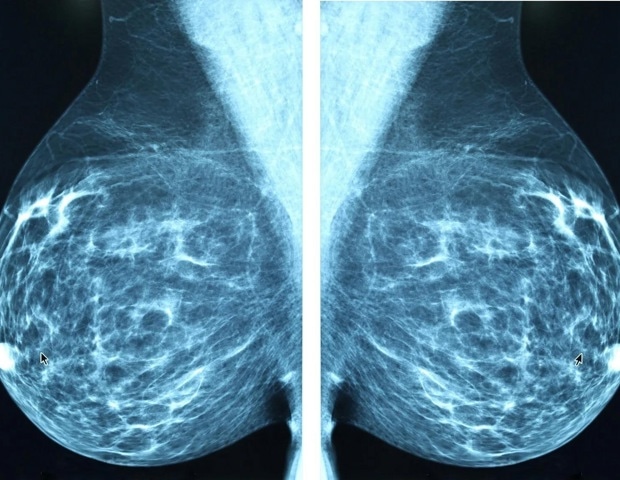
Where a woman lives significantly affects whether her breast cancer is diagnosed at an early or late stage, according to a national analysis published in the Journal of the American College of Surgeons (JACS). Researchers found…
JERUSALEM, March 11 (Xinhua) — Israeli researchers have discovered a sophisticated way in which the deadly malaria parasite keeps the host’s immune system jammed, the Weizmann Institute of Science said in a statement on Wednesday.
Their…

The disposable vapes ban in the UK could lead to young adults switching to alternative products, including cigarettes, new research led by the University of Bristol has found.
In response to rising concerns about youth vaping,…

Extreme heat is now stopping people from doing simple daily tasks like walking, cleaning, or working outside.
A new study shows that climate warming has changed how much activity the human body can safely handle in hot weather.

Insect-derived lipids are proving to be a functional and cost-effective delivery system for naturally sourced vitamin D3 that can address supply chain constraints and sustainability pressures. Nutriearth, a specialist extracting the nutrient from…
The World Health Organization (WHO) published today three new Target Product Profiles (TPPs) for antibacterial agents designed to address key drug-resistant bacteria causing severe bloodstream and urinary…

A new educational game simulates real breastfeeding complications, helping nurses learn how to spot and manage fungal nipple infections that can cause pain and early weaning.
Study: Serious game prototype for nurses on…