
Anytime global warming or climate change get mentioned online, you can expect a bunch of comments claiming to be able to disprove the whole concept, at least in relation to human activity. Most of these have been debunked, not just in detailed…
Blog
-
How AI Solved a 25-Year Crohn’s Disease Mystery
The researchers then confirmed the importance of the interaction between NOD2 and girdin by comparing mouse models of Crohn’s disease lacking the girdin protein to those with girdin intact. They found that mice without girdin…
Continue Reading
-

Trend Micro Awards Over $1,000,000 to Ethical Hackers
Participants at Pwn2Own Ireland discovered scores of zero-day vulnerabilities
DALLAS, Oct. 27, 2025 /PRNewswire/ — Trend Micro Incorporated (TYO: 4704; TSE: 4704), a global cybersecurity leader, today celebrated the…
Continue Reading
-
Clinical characteristics and prognostic analysis of concurrent Pneumocystis jirovecii pneumonia in patients with malignancies: a retrospective study | BMC Infectious Diseases
General characteristics of malignancy-PJP patients
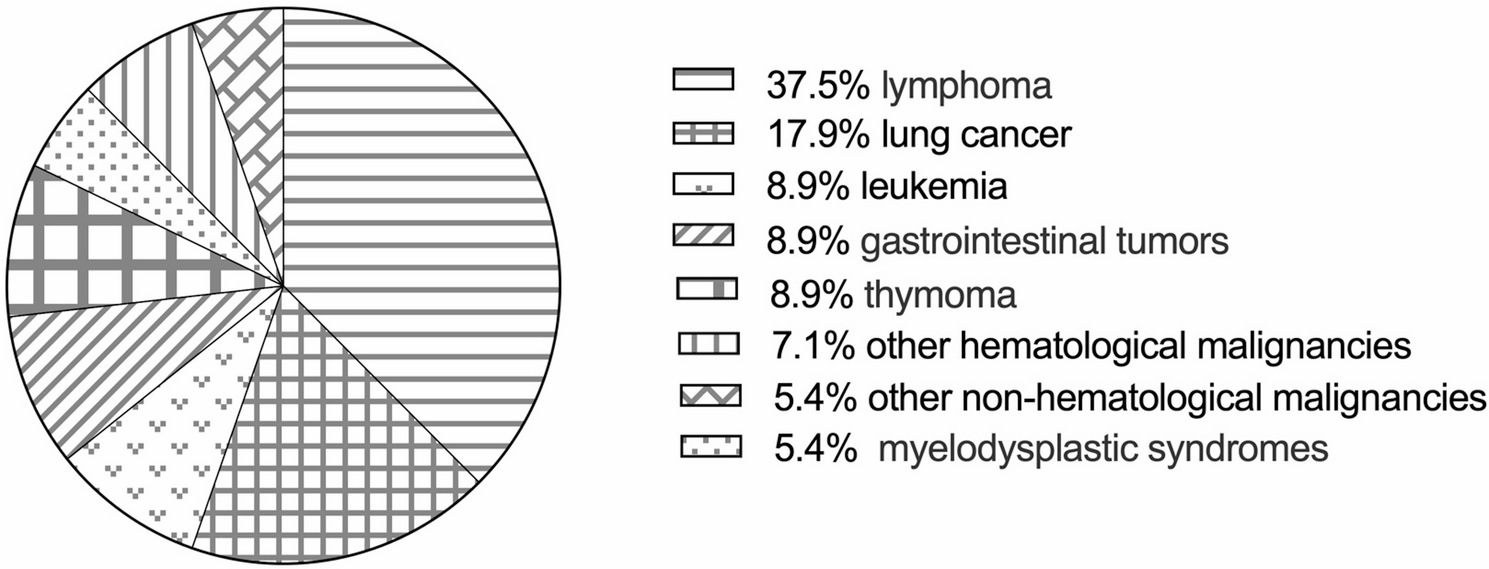
Fifty-six patients with an identified diagnosis of malignancy-PJP were enrolled in our study after a detailed medical record review. Thirty-four patients were male (60.7%), 22 patients were female (39.3%), and the mean age was 63 (52, 68) years. The underlying malignancies are shown in Fig. 1. Most patients had solid malignancies (45, 80.4%), and 11 (19.6%) had non-solid malignancies. According to the involved system, 23 (41.1%) patients had non-hematological malignancies, and 33 (58.9%) had hematological malignancies.
Fig. 1 The underlying malignancies of enrolled 56 malignancy-PJP patients. Other hematological malignancies: multiple myeloma and aplastic anemia; other non-hematological malignancies: prostate cancer, nasopharyngeal cancer, and breast cancer
The main clinical manifestations of PJP were fever (52, 92.9%), cough (47, 83.9%), expectoration (41, 73.2%), and dyspnea (47, 83.9%). Bilateral (56, 100%), ground-glass opacities (GGOs) (48, 85.7%), and patches (45, 80.4%) were the most common chest CT manifestations. Consolidations (24, 42.9%), nodular (24, 42.9%), and pleural thickening (32, 57.1%) were observed on some chest CTs of patients with malignancy-PJP. Low peripheral CD4+ T-cell [125.0 (66.0, 207.0)/µL] counts were common in patients with malignancy-PJP.
Some patients were complicated with other infections, such as CMV (25, 44.6%), bacterial HAP (23, 41.1%), oral candida infection (6, 10.7%), aspergillus infection (6, 10.7%), and Nocardia infection (2, 3.6%). Most patients experienced respiratory failure (47, 83.9%), approximately half of the patients needed intensive care unit (ICU) support, and 29 patients (51.8%) died.
After PJP diagnosis, most patients (50, 89.3%) were prescribed 15 mg/kg/d trimethoprim-sulfamethoxazole (TMP-SMX). More than one-third of our patients (21, 37.5%) were also prescribed a combination of second-line anti-PJP medications, such as caspofungin, clindamycin and primaquine.
Differences in the clinical characteristics and prognosis between PJP patients with non-hematological and hematological malignancies
According to the involved system, the 56 patients were divided into a non-hematological malignancy group and a hematological malignancy group. The differences in clinical characteristics, laboratory test results (Table 1) and imaging findings (Table 2) between the two groups were analyzed.
Table 1 The clinical characteristics between non-hematological malignancy-PJP group and hematological malignancy-PJP group Table 2 The chest CT features in non-hematological malignancy-PJP group and hematological malignancy-PJP group There were no significant differences in age, sex or comorbidities between the two groups. Compared with patients in the non-hematological malignancy group, more patients in the hematological malignancy group needed invasive mechanical ventilation support (60.6% vs. 43.5%, p = 0.03). Patients in the hematological malignancy group were more prone to respiratory failure and higher mortality, but the difference was not statistically significant. The time from diagnosis of oncological disease to PJP infection [72 (38.0, 112.5) days vs. 153 (92.5, 223.5) days, p < 0.01] and the time from chemotherapy to PJP infection [79.0 (46.5, 415.5) days vs. 229.0 (116.0, 677.5) days, p = 0.04] were shorter in the hematological malignancy group than in the non-hematological malignancy group. In terms of chest CT features, pleural thickening was more common in the non-hematological malignancy group than in the hematological malignancy group (73.9% vs. 45.5%, p = 0.03). However, there were no significant differences in the minimal albumin level, peripheral lymphocyte count or inflammatory marker levels between the two groups.
Differences between the survival and non-survival groups of patients with malignancy-PJP
The 56 patients were divided into a survival group (27 patients) and a non-survival group (29 patients) according to their clinical outcome. Compared with those in the survival group, more patients in the non-survival group were complicated with CMV (62.1% vs. 25.9%, p < 0.01) and bacterial HAP (58.6% vs. 22.2%, p < 0.01). However, there were no significant differences in clinical symptoms, chest CT features, chemotherapy before PJP infection or anti-PJP treatment between the two groups.
In terms of laboratory test results, in the non-survival group, the peripheral lymphocyte count [0.4 (0.3, 0.7) × 109/L vs. 0.8 (0.5, 1.4) × 109/L, p < 0.01], platelet count [138.0 (74.0, 197.5) × 109/L vs. 212.0 (160.8, 265.3) × 109/L, p < 0.01], minimal albumin level [21.7 ± 5.3 g/L vs. 26.6 ± 4.6 g/L, p < 0.001], T-cell count [307.0 (151.0, 377.0)/µL vs. 447.0 (245.5, 920.5)/µL, p = 0.01) and CD4+ T-cell count [123.0 (37.0, 163.0)/µL vs. 146.0 (97.0, 417.0)/µL, p = 0.03] were significantly lower than those in the survival group. However, D-dimer [8.3 (2.0, 15.6) mg/L vs. 1.9 (0.9, 6.3) mg/L, p = 0.01], high-sensitivity C-reactive protein [107.0 (36.3, 191.3) mg/L vs. 42.2 (6.9, 87.0) mg/L, p < 0.01] and lactate dehydrogenase [588.0 (441.0, 789.5) U/L vs. 319.0 (255.0, 481.0) U/L, p < 0.01] levels were greater in the non-survival group than in the survival group.
Prognostic analysis for patients with malignancy-PJP
As shown in Table 3, univariate Cox regression analysis revealed that non-solid malignancies, decreased lymphocyte count, CMV viremia, bacterial HAP, and pneumomediastinum were associated with non-survival. Subsequent multivariate Cox regression analysis revealed that non-solid malignancies (HR = 2.77, χ2 = 4.83, p = 0.03, 95% CI: 1.12–6.89), CMV viremia (HR = 3.33, χ2 = 8.93, p < 0.01, 95% CI: 1.51–7.33), bacterial HAP (HR = 2.21, χ2 = 4.10, p = 0.04, 95% CI: 1.03–4.77) and pneumomediastinum (HR = 2.50, χ2 = 3.96, p < 0.05, 95% CI: 1.01–6.14) were independent risk factors associated with poor survival in patients with malignancy-PJP.
Table 3 Univariable and multivariable Cox regression analysis of survival associated risk factors for patients with malignancy-PJP Kaplan‒Meier analysis (Fig. 2) was performed to explore the impact of the different types of underlying malignancies on the cumulative survival of malignancy-PJP patients. The results revealed that there was no significant difference in survival between patients with non-hematological malignancies and those with hematological malignancies. Compared with that of patients with solid malignancies, the survival rate of patients with non-solid malignancies (p < 0.05) was significantly lower.
Fig. 2 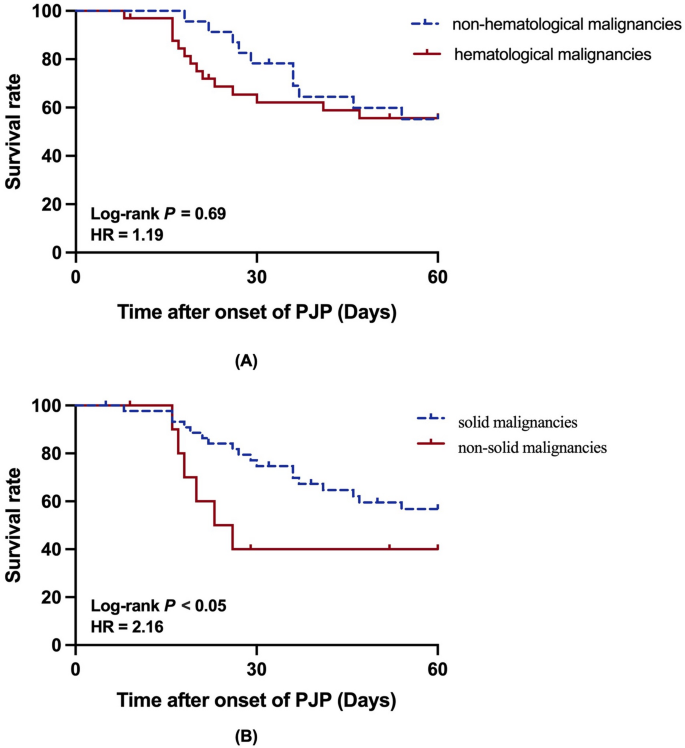
Kaplan-Meier analysis of malignancy-PJP patients on 60-day. A with hematological malignancies and with non-hematological malignancies; B with solid malignancies and with non-solid malignancies
Continue Reading
-

2025 U.S. Championships Long Track speed skating and World Cup Qualifier
As widely expected, Olympic stars Jordan Stolz, Erin Jackson, and Cooper McLeod were the standout performers at the 2025 U.S. Long Track speed skating Championships held at the Utah Olympic Oval from 24-26 October.
The event served as a…
Continue Reading
-
Jon Stewart ‘Working on Staying’ at Daily Show Amid Paramount Merger
Jon Stewart got candid about his future at “The Daily Show” at the New Yorker Festival on Sunday, telling editor David Remnick that he’s “working on staying.”
Stewart’s current contract at Comedy Central — which is now owned…
Continue Reading
-

Phil Spencer: Xbox isn’t mandating AI for creatives, and is seeing good growth in Japan
Microsoft Gaming CEO Phil Spencer has said the company’s current use of AI is chiefly for security and Xbox Live moderation, and there is no mandate for it to be used in the creative process. He separately highlighted the brand’s…
Continue Reading
-
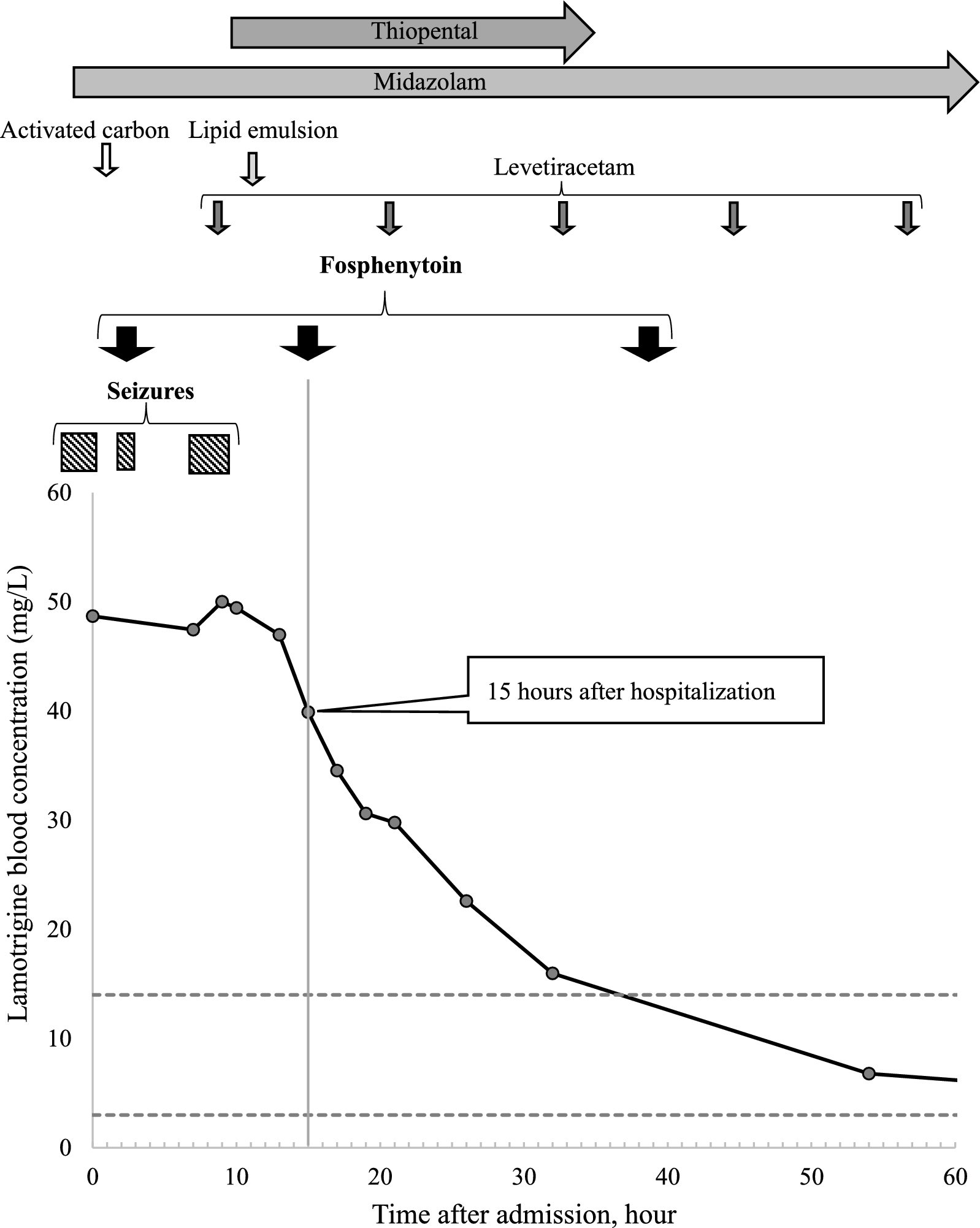
Fosphenytoin may be effective in shortening the half-life of lamotrigine in case of overdose: a case report | Journal of Medical Case Reports
The usual therapeutic dose of fosphenytoin, a prodrug of phenytoin, was administered to a patient with lamotrigine overdose who experienced seizures that did not respond to treatment with sodium bicarbonate and activated carbon. The…
Continue Reading
-

Correlation of inflammatory burden index with 30-day readmission rates in patients post-elective percutaneous coronary intervention | Journal of Cardiothoracic Surgery
Our study provides novel insights into the relationship between the IBI and the risk of 30-day readmission following elective PCI. By leveraging a comprehensive retrospective cohort, we have demonstrated that higher IBI values are significantly correlated with an increased risk of readmission, independent of traditional risk factors. This correlation was particularly pronounced in older, male patients and those with diabetes, highlighting the potential utility of IBI in risk stratification for these vulnerable populations. Our multivariate analysis revealed that a one-unit increase in IBI is associated with a 41% increase in the risk of 30-day readmission (OR 1.41, 95% CI 1.19–1.67, p < 0.001). This means that for every unit increase in IBI, the likelihood of a patient being readmitted within 30 days increases significantly. For example, a patient with an IBI of 2 compared to a patient with an IBI of 1 would have a 41% higher risk of readmission. This increased risk is likely due to the role of inflammation in promoting plaque instability, thrombus formation, and other adverse cardiovascular events that can lead to hospital readmission.
When compared to other studies, our findings are consistent with those of Li et al. [9], who demonstrated the association between inflammatory markers and the risk of hospitalization for heart failure post-myocardial infarction. However, our study extends these insights by showing that an integrated inflammatory index, rather than a single biomarker, is associated with readmission, emphasizing the complexity of inflammatory processes in cardiovascular disease [10]. The association between inflammation and cardiovascular outcomes, including post-PCI readmission, is well-established in the literature [11, 12]. Our findings are consistent with those of recent studies that have implicated inflammation in the pathogenesis of adverse cardiovascular events [13]. For instance, a study by Xie et al. [14] confirmed the predictive value of C-reactive protein, a key component of IBI, for cardiovascular events. Our study extends these insights by showing that an integrated inflammatory index, rather than a single biomarker, is associated with readmission, emphasizing the complexity of inflammatory processes in cardiovascular disease.
The potential mechanisms underlying the association between IBI and readmission are multifaceted. Inflammation is known to play a role in plaque rupture and thrombus formation, which can lead to acute coronary syndromes and potentially readmission [15]. Also, local or systemic inflammation has been proven to be a possible mechanism underlying the development of coronary slow flow phenomenon [16, 17]. Many patients experience recurrent episodes of angina due to the coronary slow flow phenomenon, leading to frequent hospitalizations [18]. Furthermore, inflammation may also contribute to the development of heart failure, a common cause of readmission following PCI [19]. By integrating multiple inflammatory biomarkers, IBI may provide a more comprehensive assessment of the inflammatory state and its impact on post-PCI outcomes.
The stronger correlation observed in older patients and those with diabetes may reflect the heightened inflammatory state often observed in these patient groups [20, 21]. Diabetes is known to induce a chronic low-grade inflammatory state, which could potentiate the association between IBI and readmission [22]. Similarly, aging is associated with an increased inflammatory burden, which may contribute to the observed association [23]. These findings underscore the importance of considering IBI in the context of patient-specific risk factors when assessing the risk of readmission. The stronger correlation observed in males may reflect sex-specific differences in inflammatory responses to PCI [24]. Emerging evidence suggests that sex hormones modulate inflammation, with males exhibiting higher levels of certain inflammatory markers compared to females [25]. This could potentially explain the enhanced association between IBI and readmission in male patients. Additionally, the higher IBI in males may also be indicative of a more aggressive inflammatory process post-PCI, which could lead to a higher likelihood of complications and subsequent readmission [26].
IL−6 is a well-established inflammatory marker that has been extensively studied in the context of cardiovascular disease. Recent studies have shown that elevated IL−6 levels are associated with increased risk of adverse outcomes following PCI. For instance, high levels of IL−6 have been linked to larger infarct sizes and higher mortality rates in patients with ST-segment elevation myocardial infarction [27]. Additionally, IL−6 has been identified as an independent predictor of non-target lesion progression in patients after coronary stenting [28]. In our study, we collected data on IL−6 levels to provide additional supporting evidence for the effectiveness of IBI. The significant difference in IL−6 levels between the readmitted and non-readmitted groups aligns with the observed trends in IBI, further validating its role as a comprehensive measure of inflammation. The inclusion of IL−6 in our data collection was intended to demonstrate that it shares a similar trend with IBI, thereby reinforcing the validity of IBI as a predictor of readmission risk.
The implications of our findings for clinical practice are significant. By identifying patients with higher IBI values as being at increased risk of readmission, clinicians may be able to target these individuals for more intensive post-discharge monitoring and intervention. This could potentially lead to a reduction in readmission rates and associated healthcare costs, as well as improved patient outcomes.
It is important to note that our study is not without limitations. As a retrospective cohort study, it is subject to the inherent biases and limitations of such designs. First, Our study is limited by the lack of standardized adjudication of readmission urgency or etiology, which precluded stratification into urgent vs. non-urgent or cardiac vs. non-cardiac categories. Future prospective studies with dedicated adjudication committees are needed to validate these findings in such contexts. Secondly, Second, geographical factors and variations in healthcare practices, as well as disparities in the availability and utilization of primary care, can significantly influence readmission rates. Our study population is drawn from a specific region, which may not be representative of other areas with different healthcare systems, patient demographics, or clinical practices. For instance, regions with limited access to primary care or specialized cardiovascular services may experience higher readmission rates due to inadequate post-discharge follow-up and management. Notably, we excluded patients who experienced major procedural complications, which were defined as complications necessitating additional interventions or treatments beyond standard PCI, such as vascular perforation, acute stent thrombosis, or significant bleeding requiring transfusion. While this exclusion was intended to focus on the elective PCI population and minimize confounding from procedures that became emergent, it may introduce selection bias. Future prospective studies are needed to validate our findings and to explore the potential of IBI as a predictive tool in a broader range of patient populations and clinical settings.
Continue Reading
-
Train like the Bodybuilders of the 80s with ‘The Weider System’
Few names carry as much weight in gym culture as Joe Weider’s. Long before lifting became the norm, Weider was lifting barbells made from scrap metal. The man behind the Mr Olympia bodybuilding competitions built the stage for stars such as a…
Continue Reading